Text size
Line height
Text spacing
Because of their unique pathophysiology, burn injuries increase the morbidity and mortality in any patient with trauma. Early intervention and resuscitation have a direct impact on survival and degree of long-term disability. A recent study involving children with burns involving more than 80% of total body surface area revealed that the major determinants of mortality include: total body surface area burned, age, inhalation injury, time to resuscitation, and the amount of initial resuscitation fluids administered (Wolfetal, 1997).
Burns cause both local lesions and systemic alterations, depending on the type and degree of the burn. The local response involves not only direct tissue coagulation, but also microvascular reactions in the surrounding dermis, resulting in extension of the injury (Aggerwal et al., 1994). Systemic response involves the release of vasoactive mediators. Thus, with burns involving more than 20% total body surface area, interstitial edema develops throughout the body due to chemical mediators and hypoproteinemia.
Airway security is the first priority during the initial evaluation. Inhalation injuries are primarily a clinical diagnosis, as many burn patients present with initially normal chest radiographs and little to no pulmonary dysfunction. Physical findings suggestive of inhalation injury include decreased mental status, evidence of respiratory distress or upper airway obstruction, carbonaceous material around the mouth or nose, singed nasal hairs, eyebrows, or eyelashes, and burns to the face and neck.
Initial Therapy of Moderate to Severe Burns
The pathophysiologic consequences of inhalation injuries include upper airway edema from direct thermal injury exacerbated by systemic capillary leak, bronchospasm from aerosolized irritants, small airway occlusion with sloughed endobronchial debris, and loss of the ciliary clearance mechanism. In addition, there can be increased dead space and intrapulmonary shunting from alveolar flooding, and decreased lung and chest wall compliance from interstitial and alveolar edema. Infection of the denuded tracheobronchial tree (tracheobronchitis) or pulmonary parenchyma (pneumonia) can occur (Sheridan, 2002).
In patients who exhibit clinical findings of inhalational injury, perform endotracheal intubation right away, because increasing edema will make later intubation difficult, if not impossible. When intubating burn patients, endotracheal tube size should be smaller than expected for the patient's size, and cricothyrotomy tools should be readily available for emergency intervention. Upper airway edema usually resolves in 2 or 3 days. This can be facilitated by elevating the head of the bed and avoiding extra fluid resuscitation for volume expansion.
Other considerations regarding smoke inhalation include exposure to carbon monoxide and more rarely hydrogen cyanide, which both block the body's ability to utilize oxygen. In the field, ventilation support of the burn patient should always include initial treatment with 100% oxygen with a non-rebreather mask. If there is suspicion of carbon monoxide exposure (altered mental status, loss of consciousness, headache, vomiting, etc.), as there often is with burns that occur in enclosed spaces, administer 100% oxygen to decrease the half-life of carboxyhemoglobin from 4.5 hours to 50 minutes. In this situation, pulse oximetry is inaccurate and oxygen saturation of the blood can only be determined by arterial blood gases. Cyanide antidote kits may be needed for cyanide poisoning.
Another issue related to pulmonary function is bronchospasm from inhaled particles and gases. This problem often responds to inhaled or intravenous bronchodilators, low dose epinephrine infusions, or parenteral steroids (Carlotto et al., 2005). High-frequency ventilators are yet another option for burn patients with extreme oxygenation failure (Schwartz et al., 1989).
Significant burns to the trunk may limit the ventilatory capacity of patients and may require escharotomies to allow the chest to expand (Thomas et al., 2003).
Due to severe capillary leak into the interstitial space in the hours following severe burns, prompt fluid resuscitation is imperative to re-expand intravascular volume, especially in patients with burns involving 15% to 20% of total body surface area. A number of studies have found that the most significant contributing factor to mortality among patients with massive burns is delay in the initiation of fluid resuscitation (Wolf et al., 1997; Kagan and Warden, 2001). Most formulas agree that half of the calculated volume should be delivered within the first 8 hours and the second half over the remaining 16 hours in a 24-hour period. Generally, the fluids within the first 24 hours should be isotonic crystalloid or lactated Ringer's solution. Colloid and blood solutions generally are not administered during the first 24 hours after a burn, but, in the case of severe burns, cautious treatment with albumin can be beneficial. The recommended resuscitation schedule is administering the least amount of fluids required for appropriate tissue perfusion and urine output of at least 1 ml/kg/hour. Two of the formulas for estimating fluid requirements are Parkland and Carvajal or Galveston. Parkland formula (Box 9) is used most often and is useful as a guide only to initiate fluid volume replacement. Subsequent replacement depends on the state of the patient and is based on the reposition of 2 to 4 ml of solution by estimated percentage of body burned multiplied by the child's body weight in kg. Parkland formula does not include maintenance therapy. Carvajal or Galveston formula, in contrast to Parkland formula, is based on body surface area instead of body weight. Therefore, in order to estimate body surface, not only the weight but also the height of the child is taken into account. This formula can be used to estimate fluid requirements when dealing with children (see Appendix)
BOX 9: Calculations of fluid needs for volume expansion
PARKLAND FORMULA
First 24 hours
Adults and children >20 kg
NOTES:
If the patiens develops hypotension, give 20 ml/kg cristalloid until normotension is achieved.
Second 24 hours, based on urine output:
Goal urine output varies depending upon the age of the patient:
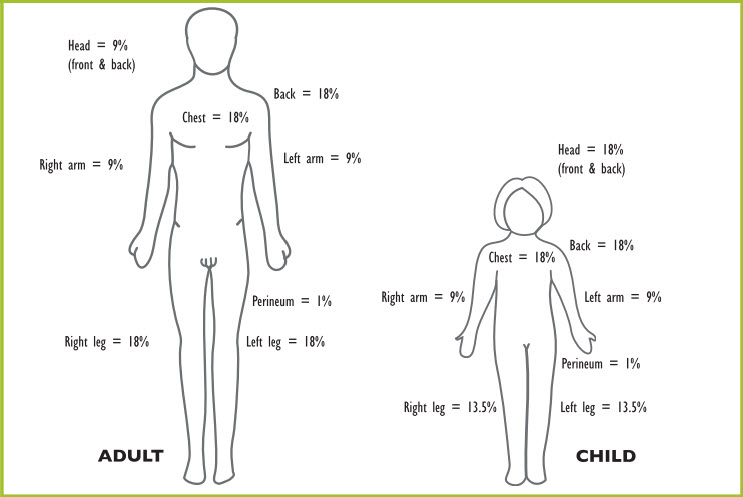
There are several charts to use. One is the rule of nines originally based on the estimation of adult body proportions, but adapted to children, as shown in Figure 12.
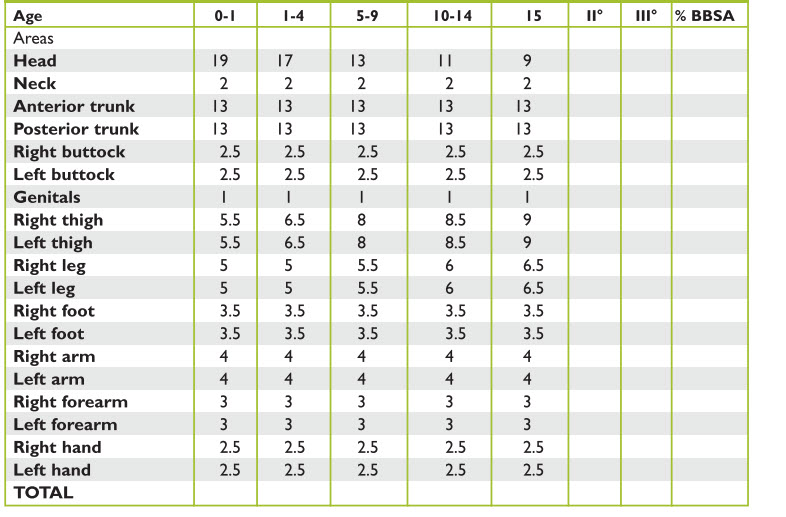
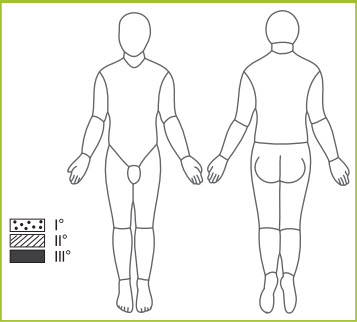
The Lund-Browder chart is an age specific chart that is used for children of up to 10 years, because it accounts for changing body proportions with age, such as the disproportioned size of the neck and head relative to lower extremities (Tables 5 and 6, Figure 13).
| Head | |
|---|---|
| 0-1 | 19 |
| 1-4 | 17 |
| 5-9 | 13 |
| 10-14 | 11 |
| 15 | 9 |
| II° | |
| III° | |
| % BBSA | |
| Neck | |
|---|---|
| 0-1 | 2 |
| 1-4 | 2 |
| 5-9 | 2 |
| 10-14 | 2 |
| 15 | 2 |
| II° | |
| III° | |
| % BBSA | |
| Anterior trunk | |
|---|---|
| 0-1 | 13 |
| 1-4 | 13 |
| 5-9 | 13 |
| 10-14 | 13 |
| 15 | 13 |
| II° | |
| III° | |
| % BBSA | |
| Posterior trunk | |
|---|---|
| 0-1 | 13 |
| 1-4 | 13 |
| 5-9 | 13 |
| 10-14 | 13 |
| 15 | 13 |
| II° | |
| III° | |
| % BBSA | |
| Right buttock | |
|---|---|
| 0-1 | 2.5 |
| 1-4 | 2.5 |
| 5-9 | 2.5 |
| 10-14 | 2.5 |
| 15 | 2.5 |
| II° | |
| III° | |
| % BBSA | |
| Left buttock | |
|---|---|
| 0-1 | 2.5 |
| 1-4 | 2.5 |
| 5-9 | 2.5 |
| 10-14 | 2.5 |
| 15 | 2.5 |
| II° | |
| III° | |
| % BBSA | |
| Genitals | |
|---|---|
| 0-1 | 1 |
| 1-4 | 1 |
| 5-9 | 1 |
| 10-14 | 1 |
| 15 | 1 |
| II° | |
| III° | |
| % BBSA | |
| Right thigh | |
|---|---|
| 0-1 | 5.5 |
| 1-4 | 6.5 |
| 5-9 | 8 |
| 10-14 | 8.5 |
| 15 | 9 |
| II° | |
| III° | |
| % BBSA | |
| Left thigh | |
|---|---|
| 0-1 | 5.5 |
| 1-4 | 6.5 |
| 5-9 | 8 |
| 10-14 | 8.5 |
| 15 | 9 |
| II° | |
| III° | |
| % BBSA | |
| Right leg | |
|---|---|
| 0-1 | 5 |
| 1-4 | 5 |
| 5-9 | 5.5 |
| 10-14 | 6 |
| 15 | 6.5 |
| II° | |
| III° | |
| % BBSA | |
| Left leg | |
|---|---|
| 0-1 | 5 |
| 1-4 | 5 |
| 5-9 | 5.5 |
| 10-14 | 6 |
| 15 | 6.5 |
| II° | |
| III° | |
| % BBSA | |
| Right foot | |
|---|---|
| 0-1 | 3.5 |
| 1-4 | 3.5 |
| 5-9 | 3.5 |
| 10-14 | 3.5 |
| 15 | 3.5 |
| II° | |
| III° | |
| % BBSA | |
| Left foot | |
|---|---|
| 0-1 | 3.5 |
| 1-4 | 3.5 |
| 5-9 | 3.5 |
| 10-14 | 3.5 |
| 15 | 3.5 |
| II° | |
| III° | |
| % BBSA | |
| Right arm | |
|---|---|
| 0-1 | 4 |
| 1-4 | 4 |
| 5-9 | 4 |
| 10-14 | 4 |
| 15 | 4 |
| II° | |
| III° | |
| % BBSA | |
| Left arm | |
|---|---|
| 0-1 | 4 |
| 1-4 | 4 |
| 5-9 | 4 |
| 10-14 | 4 |
| 15 | 4 |
| II° | |
| III° | |
| % BBSA | |
| Right forearm | |
|---|---|
| 0-1 | 3 |
| 1-4 | 3 |
| 5-9 | 3 |
| 10-14 | 3 |
| 15 | 3 |
| II° | |
| III° | |
| % BBSA | |
| Left forearm | |
|---|---|
| 0-1 | 3 |
| 1-4 | 3 |
| 5-9 | 3 |
| 10-14 | 3 |
| 15 | 3 |
| II° | |
| III° | |
| % BBSA | |
| Right hand | |
|---|---|
| 0-1 | 2.5 |
| 1-4 | 2.5 |
| 5-9 | 2.5 |
| 10-14 | 2.5 |
| 15 | 2.5 |
| II° | |
| III° | |
| % BBSA | |
| Left hand | |
|---|---|
| 0-1 | 2.5 |
| 1-4 | 2.5 |
| 5-9 | 2.5 |
| 10-14 | 2.5 |
| 15 | 2.5 |
| II° | |
| III° | |
| % BBSA | |
| TOTAL | |
|---|---|
| 0-1 | |
| 1-4 | |
| 5-9 | |
| 10-14 | |
| 15 | |
| II° | |
| III° | |
| % BBSA | |
| Areas | % Total | IIº/IIIº |
| Head / neck | ||
| Anterior trunk | ||
| Posterior trunk | ||
| Right arm / forearm | ||
| Left arm / forearm | ||
| Right buttock | ||
| Left buttock | ||
| Genitals | ||
| Right thigh | ||
| Left thigh | ||
| Right leg / foot | ||
| Left leg / foot |
The palmar surface of the hand (without fingers) can be used for second degree burns or greater, with a palm-size area equaling 0.5% to 1.0% body surface area (Kagan and Warden, 2001; Sheridan et al., 1995).
Burns can be classified according to depth. First-degree are red, dry, and painful; second-degree are red, wet, and very painful; third-degree are leathery, dry, insensitive, and waxy, and fourth-degree involve underlying tissues, tendons, and bones.
Although recommended fluid resuscitation for patients with total body surface area burns greater than 15% to 20% is by parenteral (IV) route, certain trauma or combat situations have limited resources. In light of the need for prompt initiation of fluids to decrease morbidity and mortality, several authors have suggested using oral rehydration solutions similar to lactate Ringer with the addition of glucose, or the World Health Organization's oral rehydration solution (with an osmolarity range of 260-330 mOsm/L) given orally or through nasogastric tube (Thomas et al., 2003). The drawback of oral rehydration of burn patients relates to the initially increased absorption time in comparison to intravenous fluids and the concern for poor gut function secondary to splanchnic underperfusion.
Treatment starts with stopping the burning process. Roll the child in a blanket or rug, taking care not to cover the face to avoid inhalation of fumes.
Rinse chemical burns with copious amounts of clean water.
Remove clothing and jewelry. Cool or wet dressings have no role in management of burn injuries; cover burns with a clean, dry bandage. Subsequent treatment involves cleansing and debriding loose epidermis and blisters. Topical agents that can be used include vaseline impregnated gauze, mafenide acetate cream, triple antibiotic ointment, and silver nitrate solution. More superficial wounds (involving the epidermis) and facial wounds can be dressed initially with a clean, dry dressing or with bacitracin or vaseline. Cleanse and dress deeper burns with silver sulfadiazine. Wounds treated with aqueous topical agents, especially those containing silver, are associated with secondary hyponatremia, requiring isotonic crystalloid and additional salt in enteral solutions. Careful serum sodium monitoring is imperative, because cerebral edema and seizures can occur with severe hyponatremia (Sheridan, 2002). Tetanus prophylaxis is indispensable.
Another consideration in the care of burn injuries is monitoring for signs of tissue compromise. Certain types of burns (e.g., circumferential burns of limbs, trunk, or abdomen, as well as electrical burns) are especially at risk of tissue compromise. Pain and color are unreliable markers of perfusion; generally, a warm extremity is a well-perfused extremity. Remove all constricting clothing, elevate the burned area if possible, and carefully monitor pulses. Do not wait for the development of a compartment syndrome to perform an escharotomy. Because the eschar is insensitive, escharotomies can be performed in most patients at the bedside using sedation and analgesics. Patients with large burns and generalized massive tissue edema may require intraoperative fasciotomies.