Pediatric Trauma
| Site: | Pediatric Pandemic Network Learn |
| Course: | Pediatric Trauma |
| Book: | Pediatric Trauma |
| Printed by: | Guest user |
| Date: | Sunday, June 14, 2026, 4:50 AM |
1. Overview
Welcome to this multimedia open access edition of this chapter book titled Preventive Medicine in Humanitarian Emergencies.
This content is available as a digital book in two formats:
1) Website, which you are currently reading. This format offers a mobile friendly multimedia experience with sharable links to chapters. There are three ways to move through the book:
a) Use the table of contents chapter navigation to the left to navigate to different chapters in the book. Scroll through the links to select the chapter that interests you.
b) Use the yellow arrows that appear when scrolling to select previous and next chapters.
c) Use the previous chapter and next chapter buttons at the bottom of very page to navigate through the book.
2) Printable, which you can save as a PDF and open without an Internet connection.
2. Introduction
Authors:
Joseph Wathen, MD
Lindsey Cooper, MD
Kristen Crossman, MD
Dr. Mario Acosta Bastidas
The response to a disaster situation will vary dramatically depending on the type of disaster, the number of casualties, and the ability of the affected community to respond. Preparedness to assist severely injured children is an issue of utmost importance. Few physicians are prepared to handle a large number of injured patients, much less a large number of injured pediatric patients. Personnel skilled in trauma response are essential to a successful disaster response.
Initial strategies in managing a disaster situation include: recognizing the area where the event took place, classifying injuries, and directing the affected individuals according to the severity of the injuries or damage (triage).
Assisting a pediatric population presents additional challenges, because children may not be able to talk, are overcome by fear, or they may have been separated from their families. They may also suffer lesions that the rescue personnel are not familiar with, such as crush and blast injuries or hypothermia. Providing treatment and transportation for these injured children should occur according to established priorities and available resources. Children with severe trauma often require immediate first aid before being transferred to an emergency center.
3. Response to A Disaster
oBjectives
- Emphasize the importance of safety and transportation of the wounded.
- Review the patient classification process according to the severity of the trauma and the available resources.
What Elements should a Plan for a Disaster Situation Include?
First, assume that the health care facility, wherever its location, will need to function alone until outside help arrives. It is, therefore, important to have a notification system to call in extra personnel.
It is always essential to use a triage (injured patient classification) system and to prepare adequate treatment areas to handle the influx of patients. Free up operating rooms and intensive care beds and carefully check on all available supplies (blood, medications, communication equipment). Always consider that decontamination procedures may need to be implemented as indicated. It is also necessary to ensure security in the emergency setting and to start transferring the injured people according to the priorities established through the classification process and the available resources. A public information center will be needed to distribute information to media and families. Annual drills help familiarize the staff with the disaster plans, as well as provide feedback to finetune the plans.
Available Personnel
Having a list of available personnel and appropriate means to contact them is a critical preparatory step in the face of a disaster. Arrange a central communication system that can activate a call-up roster to ensure the timely arrival of this help.
Once the personnel are at the medical facility, it becomes important to organize this labor force and provide job descriptions. A military model has been adapted to the hospital setting and is referred to as the Hospital Incident Command System (HICS). HICS has become the standard for health care disaster response and offers predictable management schemes, flexible organizational charts, prioritized response check-list, accountability of position function, and common language when communicating with outside groups.
CASE 1:
Your health care unit is sent to a neighborhood to see a child who has suffered a fall. You find an 8-year-old boy lying on the grass near a big tree. An adolescent tells you that she saw him fall from the tree when he was at a height of about 30 feet. Nobody has moved him.
Initial assessment shows that the boy is responding only to painful stimuli. Breathing is superficial with audible snoring. The skin is pale, with mild cyanosis. Respiratory rate is 12 breaths per minute; heart rate is 130 beats per minute.
The skin is cold, radial pulse is weak, and capillary refill is >3 seconds. Pupils are equally dilated and are reactive to light. Air influx cannot be detected through auscultation in the right hemithorax and is diminished in the left. Oxygen saturation is 82%.
He has broken teeth and a swollen nose, with moderate hemorrhage. The abdomen is stiff on palpation. The right leg is swollen, with evident deformity to the femur.
- Based on initial assessment and type of trauma, what are the most probable injuries in this boy?
- Analyze the initial stabilization measures and pre-hospital management of this child.
Specific Pediatric Equipment needs
Specific equipment must be available in disaster emergency situations involving children. Box 1 displays a list of recommended equipment.
BOX 1: Recommended equipment for pediatric emergencies in disaster situations
Airway Management
- Oxygen source with flow-meter
- Simple face masks – infant, child, adult
- Pediatric and adult masks for assisted ventilation
- Self-inflating bag with 250 cc, 500 cc, and 1000 cc reservoir
- Wall suctioning device or suctioning machine
- Suction catheters – Yankauer, 8, 10, 14F
- Oropharyngeal airway tubing (infant and adult sizes)
- Nasal tubing – infant, child, and adult sizes 1-3
- Optional for intubation
- Laryngoscope handle with batteries
- Miller blades – 0, 1, 2, 3
- Endotracheal tubes, uncuffed – 3.0, 3.5, 4.0, 4.5, 5.0, 6.0, cuffed – 7.0, 8.0
- Intubation guides – small, large
- Adhesive tape to secure endotracheal tube
Intravascular Access or Fluid Management
- IV catheters – 18, 20, 22, 24-gauge
- Butterfly needles – 23-gauge
- Intraosseous needles – 15- or 18-gauge
- Boards, tape, tourniquet IV
- Pediatric drip chambers and tubing
- 5% dextrose in normal saline and half normal saline
- Isotonic fluids (normal saline or lactated Ringer’s solution)
Miscellaneous
- Blood pressure cuffs – premature, infant, child, adult
- Nasogastric tubes – 8, 10, 14F
- Sphygmomanometer
- Splints and gauze padding
- Rolling carts with supplies such as abundant blankets
- Warm water source and portable showers for decontamination
- Thermal control (radiant cradle, lamps)
- Geiger counter (if suspicion of radioactive contamination)
- Personal protective equipment (PPE)
Monitoring Equipment
- Portable monitor/defibrillator (with settings <10)
- Pediatric defibrillation paddles
- Pediatric ECG skin electrode contacts (peel and stick)
- Pulse oxymeter with reusable (older children) and non-reusable (small children) sensors
- Device to check serum glucose and strips to check urine for glucose, blood, etc.
Among the recommended equipment, elements for proper airway management in children are crucial. A major challenge of any disaster response is gathering, organizing, and moving supplies to the affected area. Resource management within the hospital and other facilities or agencies may prove to be a decisive factor in whether a mass casualty event can be handled or not.
Communication
A very important aspect during a disaster situation is the ability to communicate, not only with others in the community but also among the medical personnel involved in responding to the situation. A coordinated response is needed in order to adequately handle a large influx of patients. Ideally, personal radios or cell phones should be available, so that the personnel involved in health care management communicate with each other and with the central command leader. The same applies to other areas (administration, security, maintenance).
Scene Safety and Transport
Most physicians are not trained in onscene rescue efforts. In general, local police, firefighters, and hazmat teams are the best to initially approach and control a disaster scene. However, in confined spaces, triage may need to be set up in the field and this may put the health care providers close to the disaster location.
What are the risks involved at the disaster scene?
Risks at the actual disaster scene vary according to the nature of the disaster. These include: structural instability and further collapse, fires, carbon monoxide, cyanide, dirty bombs, contamination with biologic material, and infectious agents. Other potential hazards in confined spaces include: poor air quality, airborne pollutants, toxic gases, an explosive/flammable atmosphere, and insufficient oxygen concentration (Box 2).
BOX 2: Risks at a scene of a disaster
- Structural instability and further collapse
- Fires, carbon monoxide, noxious gases such as cyanide
- Heavy dust load; insufficient oxygen
- Dirty bombs: chemical, radioactive
- Biohazard: sewage, body fluids, blood exposure
- Infectious agents
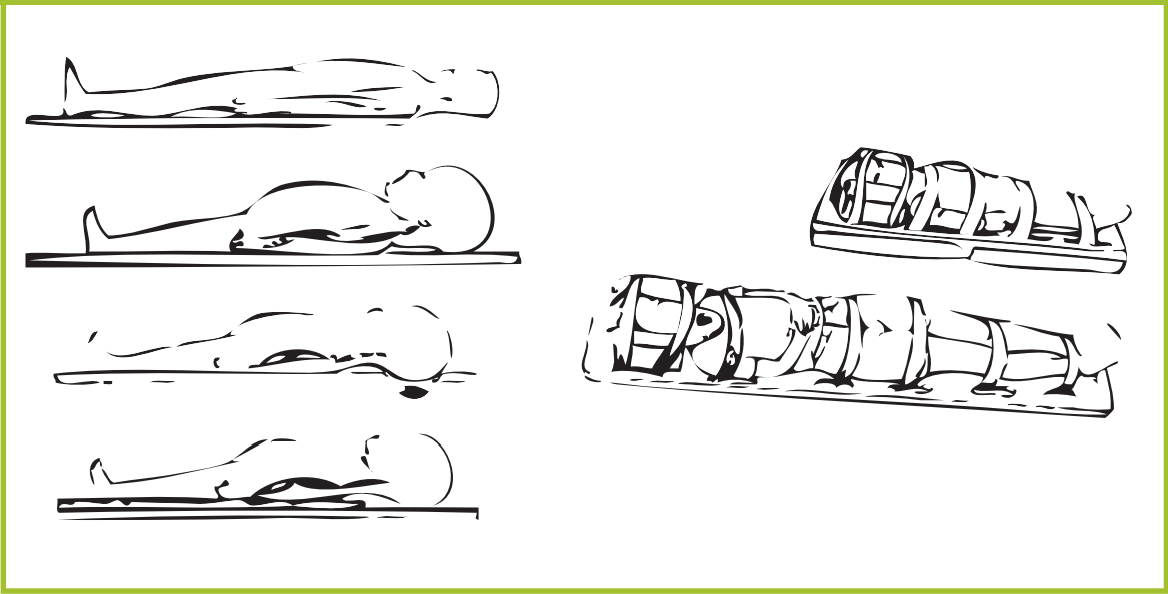
Ideally, patients will be promptly transported to a local medical clinic or hospital. The initial response at the scene of a large disaster, once the patient has been rescued, includes airway support, spine immobilization, and oxygen delivery. The increased neck flexion that occurs from the large head of small children on a backboard can be addressed with either a scooped-out head area on the backboard or with a small roll of cloth placed under the shoulders to elevate the trunk (Figure 1). Immobilization on a backboard is primarily expected to protect the spine during transport and facilitate transport. It is important to get the child off the backboard within a couple of hours.
Figure 1. Scene Immobilization
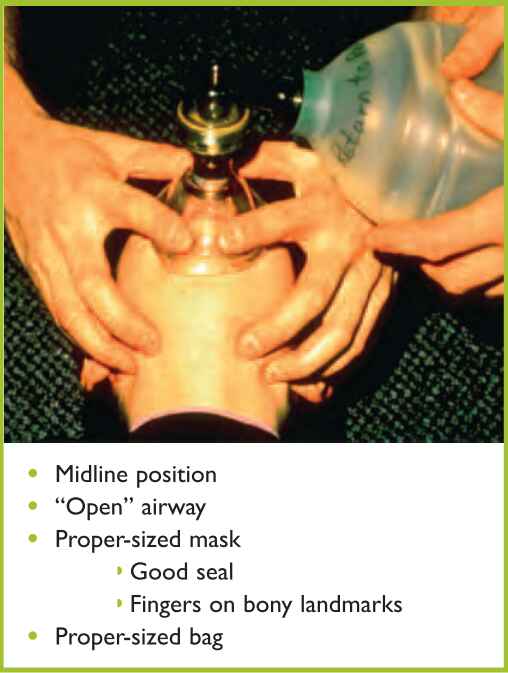
Keeping the airway open during transport of the traumatized child is a top priority. Airway support can be adequately maintained with bag-valve-mask ventilation (BVM). Intubation in children prior to transport is not necessary and has not been shown to improve outcome. In fact, endotracheal intubation can lead to delayed transport and increased morbidity due to improper tube placement or possible dislodgement of the tube during transport. A large study in children compared endotracheal intubation versus BVM in the pre-hospital setting. This study included 830 patients below age 13, randomly assigned to BVM or endotracheal intubation. Results showed that there was no advantage in placing an endotracheal tube (ETT) prior to transport to a hospital (Gausche et al., 2000). This adds to the risks that may arise from improper ETT placement. Therefore, proper BVM technique remains one of the most important skills to teach and review with local first responders to a disaster situation (Figure 2).
Figure 2. Bag-valve-mask ventilation
Injured individuals with high morbidity or mortality risk should be promptly transported. The highest level of pediatric health care is needed for falls, fires, explosions, blunt injuries, and penetrating injuries (Box 3).
BOX 3: High-risk pediatric injuries
- Falls from more than 6 m
- Fires: burns and asphyxia or highrisk burns (>10% second-degree or >5% third-degree or any burn with airway involvement)
- Explosions
- Blunt trauma: Significant injury with physiologic compromise (tachycardia with at least two signs of hypoperfusion or hypotension for age or altered mental status or spinal cord injury with neurological compromise)
- Penetrating injuries: shot, stabbing
4. Pediatric Trauma Assessment
Objectives
- Recognize the distinctive features of global management of the child with trauma.
- Assess children with trauma according to specific priorities.
- Name the most common traumatic injuries among children.
Global Management of the child with Trauma
The management of pediatric trauma requires a systematic approach. The ABCDE strategy is a widely accepted strategy for initial evaluation, stabilization, and immediate treatment if necessary, and it must then be followed by a secondary evaluation. This process usually takes place before a detailed personal history or complete physical examination data are available.
Three peaks of trauma mortality rates can be identified. The first peak corresponds to deaths within the first seconds or minutes after the traumatic event, due to serious injury to the brain, spinal cord, heart, or aortic or large vessels. Few patients are able to survive these injuries, even with immediate assistance.
The second peak in mortality rates occurs from minutes to hours after the trauma. These patients have better survival chances if they are treated during the first hours after the incident (golden hours) or, ideally, during the first hour. The injuries associated with this peak include epidural or subdural hematoma, hemothorax or tension pneumothorax, lesions with significant bleeding, such as intra-abdominal injuries (spleen laceration or rupture), and complex pelvic fractures.
Case 2
You are called to a sports field where a 6-year-old girl has been struck with a hockey stick. The girl has a large hematoma in the forehead and is crying. She has not lost consciousness, but she is not making eye contact with her teacher or with you. She looks confused, her blood pressure is normal, and the ABCDE assessment shows normal vital signs with no other apparent injuries. During the initial evaluation the girl exhibits progressive drowsiness and it is difficult to wake her.
- What is the major threat to this patient's life?
- What interventions are needed?
The third peak in trauma mortality rate occurs from days to weeks after the traumatic event and is due to multiorgan failure or sepsis.
The Advanced Trauma Life Support (ATLS) course was designed in the United States to provide health personnel with a tool for a systematic approach to the management of injured patients. In this course, emphasis is placed on management during the first critical hour. The same guidelines are used in a disaster situation that requires management of large numbers of victims. The goal with each patient is to identify and manage the most life-threatening condition using the ABCDE approach. This approach can be used with both adults and children, as long as pediatric-specific features are taken into consideration.
4.1. What are the Features Specific to Pediatric Patients?
There are specific differences between children and adults to be considered in emergency settings. Children are at a disproportionately increased risk for different reasons:
- High respiratory rate: Children are more vulnerable to aerosolized agents, chemicals, carbon monoxide, etc.
- Less fluid reserve: Children are more susceptible to dehydration.
- Less circulating volume: Smaller amounts of blood loss can lead to hypovolemic shock.
- Developmental vulnerabilities: Infants and toddlers are less able to escape a disaster; they cannot follow directions or make immediate choices.
- Anatomic and physiologic differences:
- Prominent occiput: Flexion of the neck on spine boards.
- Increased amount of secretions: May require more suctioning.
- Infants <3 months are obligate nose breathers: Susceptible to anatomic obstruction and infections.
- Relatively larger tongue compared with mandible: May make use of bagvalve-mask or intubation difficult.
- Large adenoids: Bleeding is common, especially with nasal intubations.
- Flexible omega-shaped epiglottis, with anterior location: Intubation and visualization of the larynx require lifting the epiglottis with a straight blade.
- Smaller diameter of the subglottic region until about age 8; therefore, noncuffed endotracheal tubes (ETTs) are used until ~8 years of age to avoid cuff trauma.
4.2. How is a Child with Trauma Assessed?
Assessment of pediatric trauma includes an ABCDE approach adapted to pediatric characteristics. This approach encompasses the identification and treatment of pediatric trauma, such as traumatic brain injury, respiratory and thoracic trauma, and blunt abdominal trauma (Box 4).
BOX 4: Assessment of the child with trauma
- Primary survey
- Secondary survey
- Pediatric trauma score (PTS)
Primary Survey
The primary survey is the initial evaluation of the patient, where life-threatening problems are identified and treated. It is designed to assess each of the following items in a given order (Nichols et al, 1996):
A Airway maintenance
B Breathing and ventilation
C Circulation with hemorrhage control
D Disability: neurologic status
E Exposure/environment
Airway
The goals of airway management are recognition and relief of obstruction, prevention of gastric content aspiration, and promotion of adequate gas exchange. In managing a trauma patient's airway it is important to take potential cervical spine injuries into consideration. Maintain midline positioning and perform a jaw thrust maneuver to open the airway and protect the cervical spine. In these cases, tilting the head or lifting the chin is contraindicated. Cervical spine immobilization should include a hard cervical collar.
Airway assessment determines whether the airway is stable. If necessary, perform airway maneuvers such as jaw thrust maneuvers and nasal or oral suctioning to keep the airway open. Despite these maneuvers, it may be impossible to maintain the airway. In this case, placing an ETT with rapid sequence intubation to secure the airway would be the first option, followed by a cricothyrotomy as last resort (Box 5).
BOX 5: Airway assessment in children
- Stable airway
- It is possible to maintain the airway
open- Airway opening maneuvers
- Devices: oral or nasal airway
- It is NOT possible to maintain the airway open
- Bag-Valve-Mask (BVM)
- Endotracheal tube (rapid sequence intubation)
- Cricothyrotomy
Breathing
During the primary survey, once the airway has been assessed and kept open, assessment of breathing follows for the evaluation of oxygenation and ventilation (thoracic movements, air influx, proportion of oxygen in inspired air, skin color). Some patients, such as those with pulmonary contusions, will need positive pressure ventilation. This can initially be provided using BVM ventilation until a definitive airway is obtained. New standards for assessing ventilation include the use of CO2 monitors. Finally, inspect the chest wall looking for signs of pneumothorax or evidence of other chest wall trauma.
Circulation
After airway and breathing assessment and stabilization have been completed, the next step is the assessment of circulation. Adequate circulation can be determined by assessing the pulse strength and rate both centrally and peripherally. Capillary refill, although potentially affected by environmental factors such as temperature, can also help to determine peripheral perfusion. Measure blood pressure, keeping in mind that in children compromised circulation may occur despite a normal blood pressure. Hypotension in children will not be evident until 25% to 30% of blood volume is lost.
Tachycardia is an early marker of hypovolemia in children. It represents a compensatory mechanism to blood loss and is more marked in children than in adults. Once hypotension occurs, the child is in very serious condition.
Use direct pressure on wounds to control for external hemorrhage. This includes assessing the back of the patient, as scalp injuries can be associated with significant bleeding. In general, use thin compression dressings rather than bulky dressings, so that adequate pressure to the bleeding site can be delivered. Intravenous fluid resuscitation with isotonic fluid such as lactated Ringer’s solution or normal saline should begin immediately. If blood loss has been substantial, anticipate the need for blood products such as O negative packed red blood cells, fresh frozen plasma, etc, and begin type and cross of patient and potential donors. If IV access can not be obtained, insert an intraosseous line for fluid administration.
State of Consciousness
State of consciousness is evaluated through a quick neurologic assessment. Assess whether the child is alert, responsive to verbal or painful stimuli, or unresponsive (AVPN). In addition, assess the pupils for size, equality, and response to light. A quick motor exam can determine if all four extremities show motor activity. A detailed neurologic exam can wait until the secondary survey. Some medical facilities will assign the child a score at this point using the adult/child and infant versions of the Glasgow Coma Scale (GCS) (Box 6, Tables 1 and 2). A score of 8 or lower indicates a significant neurologic disability and the risk of respiratory compromise. If your patient has a low GCS score, consider endotracheal intubation, but keep in mind the risks of tube dislodgement in transport and the resources to maintain ventilation.
BOX 6: GCS Values
- A score between 13 and 15 may indicate a mild head injury
- A score between 9 and 12 may indicate a moderate head injury
- A score ≤8 indicates a severe head injury (endotracheal intubation is usually required)
Adapted from: American College of Surgeons, Advanced Trauma Life Support: Course for Physicians, 1993.
| Table 1. Glasgow Coma Scale (adult/child) | ||
|---|---|---|
| Eyes Open | Verbal response | Motor response |
| 4. Spontaneous | 5. Oriented and speaks | 6. Obeys verbal commands |
| 3. To speech | 4. Disoriented and speaks | 5. Localizes pain |
| 2. To pain | 3. Inappropriate words | 4. Withdraws in response to pain |
| 1. Absent | 2. Incomprehensible sounds | 3. Decorticate to pain |
| 1. None | 2. Decerebrate to pain | |
| 1. No response | ||
| Table 2. Glasgow Coma Scale (infants) | ||
|---|---|---|
| Eyes Open | Verbal response | Motor response |
| 4. Spontaneous | 5. Coos and babble | 6. Moves spontaneously and purposefully |
| 3. To speech | 4. Irritable cries | 5. Withdraws to touch |
| 2. To pain | 3. Cries to pain | 4. Withdraws in response to pain |
| 1. Absent | 2. Moans to pain | 3. Flexion |
| 1. No Response | 2. Extension | |
| 1. No response | ||
Exposure/Environment
Removing clothing allows for a complete exposure and evaluation for other injuries.
Among the concerns related to environment is proper body temperature regulation. It is important to bear in mind that infants can rapidly become hypothermic, due to their large surface area-to-volume ratio. This is particularly true if the child is wet. Hypothermia alone has been shown to be an independent risk factor for mortality following major trauma (Gentilello et al, 1997). Effectiveness of rewarming has been studied; only patients treated with hot packs had an increase in body temperature, compared to passive rewarming with blankets and warmed IV fluids (Watts et al, 1999).
4.3. Secondary Survey
The secondary survey starts after the ABCDE assessment has been completed and initial management of life-threatening conditions has taken place.
Vital signs are assessed and appropriate monitors are placed as needed. The secondary survey consists of a detailed head-to-toe examination. Also included are a history of the trauma event, as well as a brief history (allergies, medications, past illnesses, last meal). Monitor the patient continuously during this survey and obtain laboratory and radiologic studies. Definitive care can begin by splinting fractures and applying wound dressings.
Finally, a staff member should provide emotional support to the child until family members are present.
4.4. Pediatric Trauma Score (PTS)
The pediatric trauma score (PTS) is used to rapidly assess the severity of the injury. This can be used to triage children and determine referral to pediatric trauma centers. It consists of six parameters that are evaluated during the initial assessment. Children with a score of 8 or less should be treated in a designated trauma center (Tables 3 and 4).
| Table 3. Pediatric trauma score (PTS) | |||
|---|---|---|---|
| Category | +2 | +1 | -1 |
| Size/weight | >20 kg | 10-20 kg | <10 kg |
| Airway | Normal | Stable | Unstable |
| Systolic BP | >90 mm Hg | 50-90 mm Hg | <50 mm Hg |
| CNS | Awake | Obtunded | Comatose |
| Open wound | None | Minor | Major |
| Fractures | None | Closed | Open or Multiple |
| Table 4. Pediatric trauma score (PTS) | |
|---|---|
| >8 | <1% mortality predicted |
| <8 | Suggests referral to trauma center |
| 4 | Predicts 50% mortality |
| <1 | Predicts >98% mortality |
Based on Tepas JJ, Alexander RH, Campbell JD, et al. An improved scoring system for assessment of the injured child. J. Trauma 1985; 25:720
4.5. What are the Most Common Traumatic Injuries in Children?
Head Injuries
Pediatric head injuries are among the most common pediatric traumatic lesions. In general, children have a thinner and more flexible skull that transfers force of trauma to the brain more intensely than in adults. Anatomically, younger children have a disproportionately larger head and weaker neck muscles than adults. When these children are involved in a trauma event, they tend to "lead with their heads." When a child presents with a significant brain injury, also known as a traumatic brain injury (TBI), consider oxygen delivery to the brain and cerebral perfusion pressure (CPP).
CPP is the difference between the mean arterial pressure and the intracranial pressure. It is important to maintain a good mean arterial pressure and to perform measures that decrease the intracranial pressure. Some measures, however, can be performed only in the intensive care setting.
When the intracranial pressure rises significantly, vital signs can be altered. Cushing's triad consists of hypertension, bradycardia, and irregular breathing pattern. In children, bradycardia is typically the first manifestation and may serve as a sign of impending brain herniation.
TBI can be classified as either primary or secondary. Primary brain injuries are those produced during trauma and may include brain contusion, diffuse axonal injury, or intracranial hemorrhage (Figure 7).
Figure 7. Types of Intracranial Hemorrhage
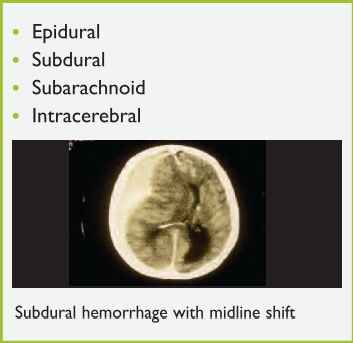
Secondary brain injuries include those that appear later as a result of metabolic effects, such as cerebral ischemia and cerebral edema. These injuries are usually seen hours to days after the traumatic event and can be minimized with proper medical care.
The management of a child that presents with a TBI begins with the ABC (airway, breathing, circulation) approach. The airway needs to be maintained with cervical spine precautions. All children should receive 100% oxygen, and intubation should be considered for GCS score <8, or for patients in whom it is not possible to maintain a stable airway. Ventilation should be assisted to maintain a PCO2 of 35 to 40 mm Hg. If there are clinical signs of brain herniation or neurologic deterioration, a lower PCO2 may be warranted.
Circulation issues include maintaining the mean arterial pressure and avoiding hypotension. Intravenous access needs to be established and either normal saline, lactated Ringer's solution, or packed red blood cells can be given. If hypotension is still present after volume expansion, cardiovascular vasopressor medication may be needed. Once the child is euvolemic, intravenous fluids can be administered at a maintenance rate.
Trauma laboratory studies and radiographs can be obtained as needed and may include serum electrolytes, glucose, complete blood count (CBC), partial thromboplastin time (PTT), prothrombin time (PT), and international normalized ratio (INR) (Significant TBI can cause coagulation alterations.). Maintain the head in a neutral position with a rigid cervical collar in place.
Provide short-term sedation and analgesia, such as midazolam (0.1 mg/kg) and fentanyl (1-2 mcg/kg) or thiopental. Thiopental reduces cerebral oxygen consumption; however, it is a cardiac depressant and can cause vasodilation. If there are clinical signs of intracranial hypertension, such as an unequal pupil dilation, abnormal posturing, or Cushing's triad, consider additional therapeutic measures including deep sedation, mannitol (0.51 g/kg), and hyperventilation (at PCO2 of 25-30 mm Hg) until clinical signs improve. Hyperventilation should be limited to serious injuries without adequate response to other interventions. Finally, consider placement of a Foley catheter and a nasogastric or oral-gastric tube in patients with severe post-traumatic brain injuries.
4.6. Thoracic Injuries
In children, thoracic injuries are associated with a high mortality rate. It is known that chest injuries cause 25% trauma deaths, mostly due to respiratory failure (Shorr et al, 1987). The greater elasticity of the ribs and sternum makes fractures less common than in adults, but there is a higher rate of energy transfer to the underlying structures (Box 7). Sternal fractures should raise the suspicion of myocardial trauma, pulmonary contusion, and great vessel injury.
BOX 7: Frequency of thoracic injuries in pediatric trauma
- Pulmonary contusion/laceration (53%)
- Pneumothorax/hemothorax (38%)
- Rib/sternum fractures (36%)
- Other lesions
- Cardiac (5%)
- Diaphragm (2%)
- Major blood vessels (1%)
From: Kassis K, Grady M. Trauma and burns in Johns Hopkins. In: Gunn VL, Nechyba C, eds. The Harriet Lane handbook: a manual for pediatric house officers, 16th ed. St. Louis: Mosby, 2002:79-94
Pulmonary contusions are the most frequent type of injury occurring with thoracic trauma. They are often missed because the initial clinical findings can be subtle. A pulmonary contusion is essentially a bruise of the lung that leads to alveolar hemorrhage and interstitial hemorrhage and edema. The severity is related to the extent of lung tissue involved. Clinical signs and symptoms include soft tissue marks on the chest, tachypnea, use of accessory respiratory muscles, and hypoxia. Continuous pulse oximetry is needed, as well as blood gas evaluation to assess the degree of PaO2 reduction and PaCO2 increase whenever possible. It is possible that decisions on ventilator management will need to be made clinically based on chest wall movement, breath sounds, and oximetry. Treatment of lung contusions consist of oxygen therapy, close monitoring, and possibly endotracheal intubation with positive end-expiratory pressure (PEEP) to help tamponade bleeding.
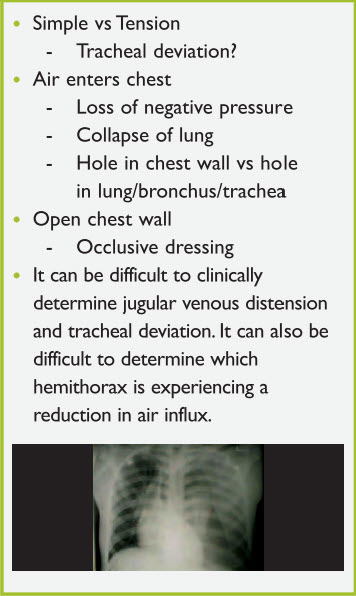
In all pneumothoraces, air enters the pleural space resulting in loss of negative pressure and lung collapse. Air may enter either through a hole in the chest wall or a hole in the lung, bronchus, or trachea. An open pneumothorax exists when there is an opening in the chest wall. Immediate treatment of such a condition consists of applying an occlusive dressing. Pneumothorax can either be simple or under tension. Assessment of the trachea helps differentiate between the two. Tension pneumothorax is a clinical diagnosis made by tracheal deviation away from the side of the pneumothorax, absent breath sounds, hypotension, and possibly distended neck veins. In young children, it may be difficult to clinically determine jugular venous distension and tracheal deviation. Tension pneumothorax is a clinical diagnosis requiring immediate needle decompression at the second intercostal space along the mid-clavicular line or placement of a chest tube in the fourth to fifth intercostal space along the mid-axillary line (Figure 8).
Figure 8. Pneumothorax
Hemothorax occurs when blood accumulates in the pleural space, which can then compress the lung. A massive hemothorax indicates a large lung injury with potential involvement of large vessels (Figure 9).
Figure 9. Hemothorax
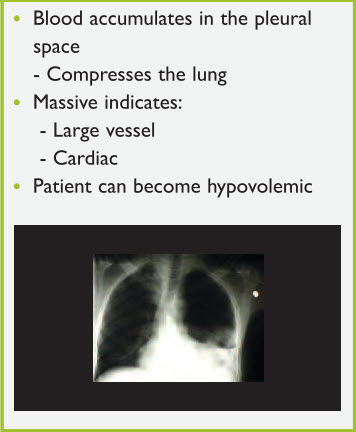
Draining the blood from the chest with a chest tube (posterior location) and treating the hypovolemia are the keys to therapy.
Pericardial tamponade presents when fluid accumulates in the pericardial sac. In trauma, this fluid is blood and usually develops over minutes to hours. This fluid causes a restriction on the myocardium leading to decreased cardiac output and hampered venous return. Clinically, Beck's triad suggests pericardial tamponade: reduced pulse pressure, neck vein distension, and muffled heart tones. Arrhythmias can be present including bradycardia, pulseless electrical activity (PEA), and asystole. The treatment includes pericardiocentesis and intravenous fluids. Clinical suspicion should arise when a penetrating trauma to the trunk has occurred. Look for soft tissue marks, such as entry site of a penetrating object and bruises across the chest wall.
4.7. Abdominal Trauma
Abdominal injuries are the third leading cause of traumatic death in children, after head and thoracic injuries.
Abdominal injuries can affect solid or hollow organs. The most common injury is that of the spleen. In general, the abdomen represents a site of "silent" hypovolemia. Other sites of silent hemorrhage that can be responsible for hypovolemia are the pelvis and the retroperitoneum.
Recognition of increasing abdominal distension, peritoneal signs, and progressive hypotension despite fluid resuscitation are signs of impending hemodynamic compromise, and indicate the need for surgical intervention. The FAST trauma scan examining 4 major quadrants with ultrasound guidance is a skill that can be acquired by emergency first responders. Blood in the right upper quadrant close to the liver is one of the most sensitive locations to look for blood. It is possible to estimate the degree of the hemoperitoneum: 1=minimal, 2=moderate, 3= large hemoperitoneum requiring surgical intervention.
Paramount to treatment is fluid and/or packed red blood cell replacement with constant reassessments of the patient's hemodynamic status. For most patients this treatment will be sufficient; surgical hemostasis is rarely needed. The unique features of the abdomen in children include a thin abdominal wall, a decreased AP diameter, increased lordosis, proportionately larger spleen and liver, exposition below the rib cage, and a kidney that is more anterior with less perinephric fat.
4.8. Extremity Trauma
Extremity trauma is very common. Fractures of the radius, ulna, and femur are most common and may be either open or closed. Always assess the neurovascular status. Initial management of extremity trauma includes recognition, splinting, neurovascular assessment, and pain control.
If there is an open wound, first clean it and then cover it. Different types of splinting devices can be used. At the scene of the disaster, use whatever is available (wood, magazines, the other leg). Once at the medical facility, fiber-glass splints are ideal as they are stronger and more water-resistant than plaster (Box 8).
BOX 8: Keys to proper splinting
- Cleaning and bandaging skin wounds prior to splinting
- Padding in layers prior to adding the splint, with extra padding at pressure points
- Making sure to splint the joint above and below the fracture
Femur fractures will also benefit from traction because of the larger muscle groups involved. Treat patients for pain and sedate them with narcotics, sedatives, and muscle relaxants.
Open fractures have the added concern of infection in addition to the medical management. Open fractures also imply that a significant force has been involved. It is therefore important to look for other injuries. In addition to infection, other complications of open fractures include nerve entrapment and compression. Treatment of an open fracture includes cleaning, covering the opening without suturing, intravenous antibiotics, and immobilization. Ideally, these injuries will need surgical debridement (Figure 10).
Figure 10. Open fractures

Pelvic fractures are a concern because they are generally the result of high-impact blunt trauma; blood loss can be significant. The pelvic ring may be fractured in a single place, which would be a stable fracture, or more commonly in multiple places, which could be an unstable fracture. Additional injuries associated with pelvic fractures include genitourinary and abdominal lesions, and vascular abnormalities (i.e. pelvic vein disruption). A sheet tightly wrapped around the pelvis may be the only temporizing measure for the unstable, bleeding pelvic fracture (Figure 11) until operative treatment is arranged.
Figure 11. Hip fracture

Fractures that need orthopedic referral include those that affect joints or growth plates, fractures around the elbow or knee with significant soft tissue swelling (compartment syndrome concern), open pelvic fractures (associated with hemorrhage) and fractures associated with an open wound or with signs of vascular or nerve disruption.
5. Disaster Specific Traumatic Injuries
Objectives
- Establish specific care procedures for victims of fires and burns in general.
- Emphasize the characteristics of injuries caused by bombs or blasts and their initial treatment.
- Characterize the crush syndrome, its consequences and treatment.
Burn Injuries
Because of their unique pathophysiology, burn injuries increase the morbidity and mortality in any patient with trauma. Early intervention and resuscitation have a direct impact on survival and degree of long-term disability. A recent study involving children with burns involving more than 80% of total body surface area revealed that the major determinants of mortality include: total body surface area burned, age, inhalation injury, time to resuscitation, and the amount of initial resuscitation fluids administered (Wolfetal, 1997).
Pathophysiology
Burns cause both local lesions and systemic alterations, depending on the type and degree of the burn. The local response involves not only direct tissue coagulation, but also microvascular reactions in the surrounding dermis, resulting in extension of the injury (Aggerwal et al., 1994). Systemic response involves the release of vasoactive mediators. Thus, with burns involving more than 20% total body surface area, interstitial edema develops throughout the body due to chemical mediators and hypoproteinemia.
Airway security is the first priority during the initial evaluation. Inhalation injuries are primarily a clinical diagnosis, as many burn patients present with initially normal chest radiographs and little to no pulmonary dysfunction. Physical findings suggestive of inhalation injury include decreased mental status, evidence of respiratory distress or upper airway obstruction, carbonaceous material around the mouth or nose, singed nasal hairs, eyebrows, or eyelashes, and burns to the face and neck.
Initial Therapy of Moderate to Severe Burns
- Remove all clothing.
- Assess burn size and severity.
- Cool down burnt areas with sterile water.
- Keep the patient warm to avoid hypothermia.
- Early rapid sequence intubation in case of inhalational injury.
- Volume expansion based on Parkland formula. (See Appendix for additional option
- Assess the need for escharotomy.
- Watch for signs of rhabdomyolysis.
- Cover all burnt areas with dry, sterile dressings.
- Transfer to a burn center.
The pathophysiologic consequences of inhalation injuries include upper airway edema from direct thermal injury exacerbated by systemic capillary leak, bronchospasm from aerosolized irritants, small airway occlusion with sloughed endobronchial debris, and loss of the ciliary clearance mechanism. In addition, there can be increased dead space and intrapulmonary shunting from alveolar flooding, and decreased lung and chest wall compliance from interstitial and alveolar edema. Infection of the denuded tracheobronchial tree (tracheobronchitis) or pulmonary parenchyma (pneumonia) can occur (Sheridan, 2002).
In patients who exhibit clinical findings of inhalational injury, perform endotracheal intubation right away, because increasing edema will make later intubation difficult, if not impossible. When intubating burn patients, endotracheal tube size should be smaller than expected for the patient's size, and cricothyrotomy tools should be readily available for emergency intervention. Upper airway edema usually resolves in 2 or 3 days. This can be facilitated by elevating the head of the bed and avoiding extra fluid resuscitation for volume expansion.
Other considerations regarding smoke inhalation include exposure to carbon monoxide and more rarely hydrogen cyanide, which both block the body's ability to utilize oxygen. In the field, ventilation support of the burn patient should always include initial treatment with 100% oxygen with a non-rebreather mask. If there is suspicion of carbon monoxide exposure (altered mental status, loss of consciousness, headache, vomiting, etc.), as there often is with burns that occur in enclosed spaces, administer 100% oxygen to decrease the half-life of carboxyhemoglobin from 4.5 hours to 50 minutes. In this situation, pulse oximetry is inaccurate and oxygen saturation of the blood can only be determined by arterial blood gases. Cyanide antidote kits may be needed for cyanide poisoning.
Another issue related to pulmonary function is bronchospasm from inhaled particles and gases. This problem often responds to inhaled or intravenous bronchodilators, low dose epinephrine infusions, or parenteral steroids (Carlotto et al., 2005). High-frequency ventilators are yet another option for burn patients with extreme oxygenation failure (Schwartz et al., 1989).
Significant burns to the trunk may limit the ventilatory capacity of patients and may require escharotomies to allow the chest to expand (Thomas et al., 2003).
Circulation
Due to severe capillary leak into the interstitial space in the hours following severe burns, prompt fluid resuscitation is imperative to re-expand intravascular volume, especially in patients with burns involving 15% to 20% of total body surface area. A number of studies have found that the most significant contributing factor to mortality among patients with massive burns is delay in the initiation of fluid resuscitation (Wolf et al., 1997; Kagan and Warden, 2001). Most formulas agree that half of the calculated volume should be delivered within the first 8 hours and the second half over the remaining 16 hours in a 24-hour period. Generally, the fluids within the first 24 hours should be isotonic crystalloid or lactated Ringer's solution. Colloid and blood solutions generally are not administered during the first 24 hours after a burn, but, in the case of severe burns, cautious treatment with albumin can be beneficial. The recommended resuscitation schedule is administering the least amount of fluids required for appropriate tissue perfusion and urine output of at least 1 ml/kg/hour. Two of the formulas for estimating fluid requirements are Parkland and Carvajal or Galveston. Parkland formula (Box 9) is used most often and is useful as a guide only to initiate fluid volume replacement. Subsequent replacement depends on the state of the patient and is based on the reposition of 2 to 4 ml of solution by estimated percentage of body burned multiplied by the child's body weight in kg. Parkland formula does not include maintenance therapy. Carvajal or Galveston formula, in contrast to Parkland formula, is based on body surface area instead of body weight. Therefore, in order to estimate body surface, not only the weight but also the height of the child is taken into account. This formula can be used to estimate fluid requirements when dealing with children (see Appendix)
BOX 9: Calculations of fluid needs for volume expansion
PARKLAND FORMULA
First 24 hours
Adults and children >20 kg
- Lactated Ringer: 2-4 mL/kg/%burn/24 hours (half in first 8 hours and the other half in following 16 hours)
- Colloid: none
NOTES:
If the patiens develops hypotension, give 20 ml/kg cristalloid until normotension is achieved.
Second 24 hours, based on urine output:
- <1 mL/kg/hour: 20 mL/kg cristalloid solution
- 1-3 mL/kg/hour: continue with Parkland formula
- >3 mL/kg/hour: reduce to 2/3 of initial formula
Goal urine output varies depending upon the age of the patient:
- Adults: 0.5 mL/kg/hour
- Children: 1 mL/kg/hour
- Infants: 1-2 mL/kg/hour
Estimation of Burn Extent
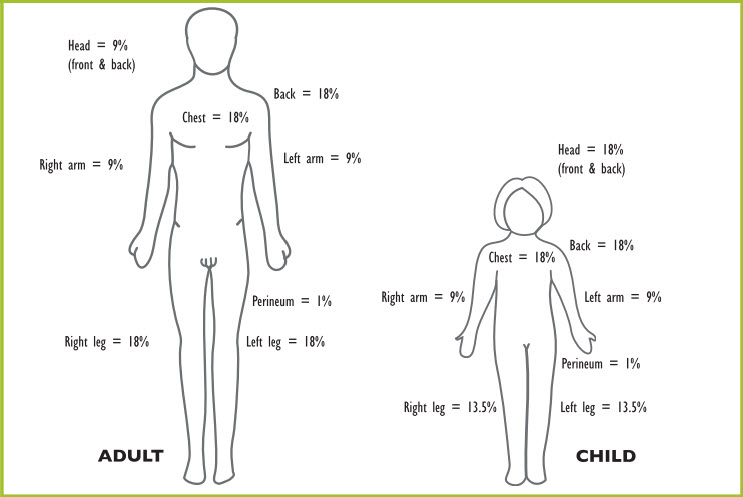
There are several charts to use. One is the rule of nines originally based on the estimation of adult body proportions, but adapted to children, as shown in Figure 12.
Figure 12. Rule of nines and adjustments for pediatric patients
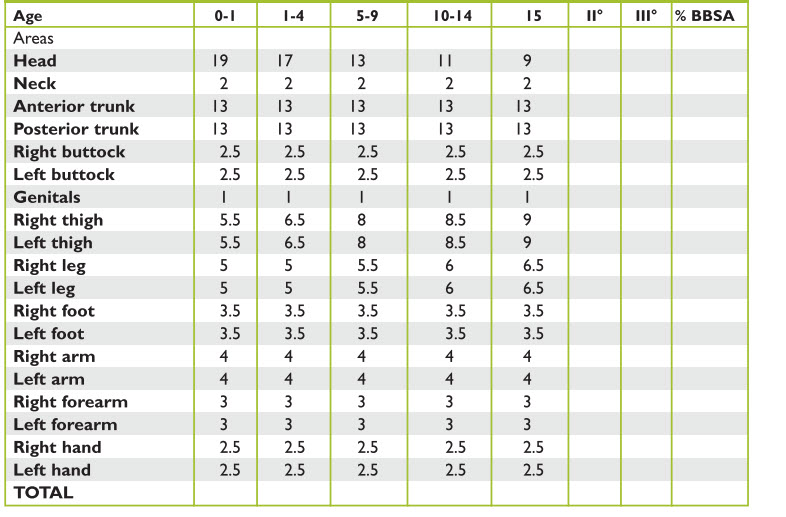
The Lund-Browder chart is an age specific chart that is used for children of up to 10 years, because it accounts for changing body proportions with age, such as the disproportioned size of the neck and head relative to lower extremities (Tables 5 and 6, Figure 13).
TABLE 5. Burn estimation (age vs. area)
| Head | |
|---|---|
| 0-1 | 19 |
| 1-4 | 17 |
| 5-9 | 13 |
| 10-14 | 11 |
| 15 | 9 |
| II° | |
| III° | |
| % BBSA | |
| Neck | |
|---|---|
| 0-1 | 2 |
| 1-4 | 2 |
| 5-9 | 2 |
| 10-14 | 2 |
| 15 | 2 |
| II° | |
| III° | |
| % BBSA | |
| Anterior trunk | |
|---|---|
| 0-1 | 13 |
| 1-4 | 13 |
| 5-9 | 13 |
| 10-14 | 13 |
| 15 | 13 |
| II° | |
| III° | |
| % BBSA | |
| Posterior trunk | |
|---|---|
| 0-1 | 13 |
| 1-4 | 13 |
| 5-9 | 13 |
| 10-14 | 13 |
| 15 | 13 |
| II° | |
| III° | |
| % BBSA | |
| Right buttock | |
|---|---|
| 0-1 | 2.5 |
| 1-4 | 2.5 |
| 5-9 | 2.5 |
| 10-14 | 2.5 |
| 15 | 2.5 |
| II° | |
| III° | |
| % BBSA | |
| Left buttock | |
|---|---|
| 0-1 | 2.5 |
| 1-4 | 2.5 |
| 5-9 | 2.5 |
| 10-14 | 2.5 |
| 15 | 2.5 |
| II° | |
| III° | |
| % BBSA | |
| Genitals | |
|---|---|
| 0-1 | 1 |
| 1-4 | 1 |
| 5-9 | 1 |
| 10-14 | 1 |
| 15 | 1 |
| II° | |
| III° | |
| % BBSA | |
| Right thigh | |
|---|---|
| 0-1 | 5.5 |
| 1-4 | 6.5 |
| 5-9 | 8 |
| 10-14 | 8.5 |
| 15 | 9 |
| II° | |
| III° | |
| % BBSA | |
| Left thigh | |
|---|---|
| 0-1 | 5.5 |
| 1-4 | 6.5 |
| 5-9 | 8 |
| 10-14 | 8.5 |
| 15 | 9 |
| II° | |
| III° | |
| % BBSA | |
| Right leg | |
|---|---|
| 0-1 | 5 |
| 1-4 | 5 |
| 5-9 | 5.5 |
| 10-14 | 6 |
| 15 | 6.5 |
| II° | |
| III° | |
| % BBSA | |
| Left leg | |
|---|---|
| 0-1 | 5 |
| 1-4 | 5 |
| 5-9 | 5.5 |
| 10-14 | 6 |
| 15 | 6.5 |
| II° | |
| III° | |
| % BBSA | |
| Right foot | |
|---|---|
| 0-1 | 3.5 |
| 1-4 | 3.5 |
| 5-9 | 3.5 |
| 10-14 | 3.5 |
| 15 | 3.5 |
| II° | |
| III° | |
| % BBSA | |
| Left foot | |
|---|---|
| 0-1 | 3.5 |
| 1-4 | 3.5 |
| 5-9 | 3.5 |
| 10-14 | 3.5 |
| 15 | 3.5 |
| II° | |
| III° | |
| % BBSA | |
| Right arm | |
|---|---|
| 0-1 | 4 |
| 1-4 | 4 |
| 5-9 | 4 |
| 10-14 | 4 |
| 15 | 4 |
| II° | |
| III° | |
| % BBSA | |
| Left arm | |
|---|---|
| 0-1 | 4 |
| 1-4 | 4 |
| 5-9 | 4 |
| 10-14 | 4 |
| 15 | 4 |
| II° | |
| III° | |
| % BBSA | |
| Right forearm | |
|---|---|
| 0-1 | 3 |
| 1-4 | 3 |
| 5-9 | 3 |
| 10-14 | 3 |
| 15 | 3 |
| II° | |
| III° | |
| % BBSA | |
| Left forearm | |
|---|---|
| 0-1 | 3 |
| 1-4 | 3 |
| 5-9 | 3 |
| 10-14 | 3 |
| 15 | 3 |
| II° | |
| III° | |
| % BBSA | |
| Right hand | |
|---|---|
| 0-1 | 2.5 |
| 1-4 | 2.5 |
| 5-9 | 2.5 |
| 10-14 | 2.5 |
| 15 | 2.5 |
| II° | |
| III° | |
| % BBSA | |
| Left hand | |
|---|---|
| 0-1 | 2.5 |
| 1-4 | 2.5 |
| 5-9 | 2.5 |
| 10-14 | 2.5 |
| 15 | 2.5 |
| II° | |
| III° | |
| % BBSA | |
| TOTAL | |
|---|---|
| 0-1 | |
| 1-4 | |
| 5-9 | |
| 10-14 | |
| 15 | |
| II° | |
| III° | |
| % BBSA | |
TABLE 6. Burn assessment
| Areas | % Total | IIº/IIIº |
| Head / neck | ||
| Anterior trunk | ||
| Posterior trunk | ||
| Right arm / forearm | ||
| Left arm / forearm | ||
| Right buttock | ||
| Left buttock | ||
| Genitals | ||
| Right thigh | ||
| Left thigh | ||
| Right leg / foot | ||
| Left leg / foot |
Figure 13. Lund-Browder Chart
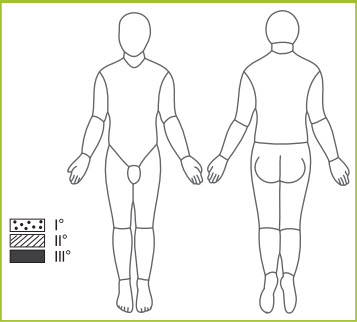
The palmar surface of the hand (without fingers) can be used for second degree burns or greater, with a palm-size area equaling 0.5% to 1.0% body surface area (Kagan and Warden, 2001; Sheridan et al., 1995).
Burns can be classified according to depth. First-degree are red, dry, and painful; second-degree are red, wet, and very painful; third-degree are leathery, dry, insensitive, and waxy, and fourth-degree involve underlying tissues, tendons, and bones.
Oral Rehydration
Although recommended fluid resuscitation for patients with total body surface area burns greater than 15% to 20% is by parenteral (IV) route, certain trauma or combat situations have limited resources. In light of the need for prompt initiation of fluids to decrease morbidity and mortality, several authors have suggested using oral rehydration solutions similar to lactate Ringer with the addition of glucose, or the World Health Organization's oral rehydration solution (with an osmolarity range of 260-330 mOsm/L) given orally or through nasogastric tube (Thomas et al., 2003). The drawback of oral rehydration of burn patients relates to the initially increased absorption time in comparison to intravenous fluids and the concern for poor gut function secondary to splanchnic underperfusion.
What is the Initial Wound care for Burn Injuries?
Treatment starts with stopping the burning process. Roll the child in a blanket or rug, taking care not to cover the face to avoid inhalation of fumes.
Rinse chemical burns with copious amounts of clean water.
Remove clothing and jewelry. Cool or wet dressings have no role in management of burn injuries; cover burns with a clean, dry bandage. Subsequent treatment involves cleansing and debriding loose epidermis and blisters. Topical agents that can be used include vaseline impregnated gauze, mafenide acetate cream, triple antibiotic ointment, and silver nitrate solution. More superficial wounds (involving the epidermis) and facial wounds can be dressed initially with a clean, dry dressing or with bacitracin or vaseline. Cleanse and dress deeper burns with silver sulfadiazine. Wounds treated with aqueous topical agents, especially those containing silver, are associated with secondary hyponatremia, requiring isotonic crystalloid and additional salt in enteral solutions. Careful serum sodium monitoring is imperative, because cerebral edema and seizures can occur with severe hyponatremia (Sheridan, 2002). Tetanus prophylaxis is indispensable.
Another consideration in the care of burn injuries is monitoring for signs of tissue compromise. Certain types of burns (e.g., circumferential burns of limbs, trunk, or abdomen, as well as electrical burns) are especially at risk of tissue compromise. Pain and color are unreliable markers of perfusion; generally, a warm extremity is a well-perfused extremity. Remove all constricting clothing, elevate the burned area if possible, and carefully monitor pulses. Do not wait for the development of a compartment syndrome to perform an escharotomy. Because the eschar is insensitive, escharotomies can be performed in most patients at the bedside using sedation and analgesics. Patients with large burns and generalized massive tissue edema may require intraoperative fasciotomies.
5.1. Special Situations
Electrical Injury
Low-and intermediate-voltage exposures can cause locally destructive injuries, as well as systemic complications. High-voltage exposures cause delayed neurologic and ocular sequelae. It is necessary to serially examine injured extremities for intracompartmental edema requiring decompression. Place bladder catheters to document and treat myoglobinuria.
Chemical Injury
Irrigate the wounds with abundant clean water (isotonic crystalloid for eye globe injuries). Close monitoring of electrolytes is necessary.
Tar Injury
Water irrigation is initially needed to cool molten tar and stop the burning process. Then, remove the cooled tar with lipophylic solvent during the debriding process.
Overall, prompt management of burn patients—with careful monitoring of airway, fluids and electrolytes, and clinical status—will directly impact morbidity and mortality. Definitive management will be determined by the degree of injury, concomitant injuries, and availability of resources.
In a disaster situation with many burned victims and poor resources, priority should be given to admitting children with a burned surface area of more than 10%, those having the face, the hands, the feet and the perineum burned, those having joints burned and circumferential injuries, and those that can't be treated out of hospital for these or other injuries. It is wise to try to establish at least one IV access in patients with burns of more than 10% body surface areas and start fluid replacement with crystalloid 20 ml/kg.
Burns affecting the airway need on site urgent interventions, such as protection of the airway and fluid administration.
Pain should be managed with painkillers and sedatives, titrating doses to the desired effect. The patient should be transferred as soon as possible. When transportation is delayed or prolonged, consult the Burn Department of the reference hospital to establish the rate of intravenous fluid replacement.
Blast Injury
Bombs and explosives can cause distinctive injuries. Survivors of an explosion typically suffer both penetrating and blunt trauma injuries. Blast lung is the most common lethal injury. Half of all initial casualties will seek medical care over a one-hour period.
The upside-down triage triangle (▽) is a reminder that the least sick will arrive at the hospital first, whereas those who are sicker, trapped, closer to the explosion site, or unable to ambulate will arrive later after rescue and in smaller numbers.
Explosives can be classified as either high-order (HE) or low-order (LE). Highorder explosives, such as TNT, C-4, nitroglycerin, or ammonium cause a supersonic over-pressurization shock wave. Loworder explosives, such as black powder or nitrocellulose cause a subsonic explosion.
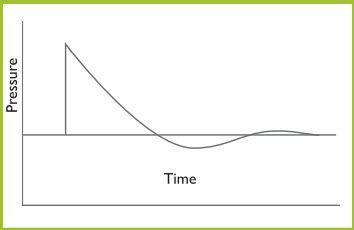
Most of the injuries seen after HE detonations are blunt, penetrating, and thermal trauma. Soft-tissue and head injuries are the most common injuries. Orthopedic injuries are also common. Primary blast injury is a less common, often subtle or delayed potentially life-threatening problem that must be considered. It is a result of abrupt pressure changes generated by the blast wave. As the Friedlander curve shows, a blast wave generates a shock wave that expands spherically. There is an instantaneous rise to a peak over-pressure that declines exponentially to an under-pressure (zone behind the high-pressure blast) (Figure 14). The rapid pressure change is the cause of the primary blast injury. Both high -and low- pressure changes can cause injury.
Figure 14. Friedlander Curve
5.2. What Types of Injuries are Associated with Blast Trauma?
Primary Injury
Primary injury is the result of the excessive pressure generated by the blast wave. It affects all air or fluid filled cavities (lungs, ears, gastrointestinal tract). It may cause air embolism resulting in a stroke or in acute abdominal or spinal cord injury.
Secondary Injury
Secondary injuries are caused by pieces of flying debris that act as projectiles, resulting in penetrating or blunt injuries. About 10% of these are eye injuries.
Tertiary Injury
Tertiary injuries occur when the body is thrown by the blast wind and may include fractures, brain injuries, traumatic amputations and other injuries.
Quaternary Injuries
Quaternary trauma injuries include all other blast trauma injuries such as burns, crush injuries, respiratory (dust/ toxins) injuries, and others.
Blast Lung Injuries
Blast lung is the most common primary blast injury among victims of explosions. It may appear up to 48 hours after the explosion. The acceleration/deceleration process may tear the lung parenchyma off the stationary vascular tree, causing hemorrhage and air emboli. Lung injury may also be induced by smoke inhalation; symptoms include dyspnea, cough, hemoptysis, chest pain, and hypoxia. The initial triad of apnea, bradycardia, and hypotension may occur. Pulmonary injuries that may occur vary from petechiae to pulmonary hemorrhage.
In general, primary blast injury of the lung is manifested as pulmonary contusion. The development of respiratory symptoms and hypoxia may occur in either a fulminant pattern or gradually over the first 48 hours.
Other potential injuries include bronchopleural fistula or arterial air embolism that may be associated with low vascular pressures after hemorrhage or high airway pressures during resuscitation with positive pressure ventilation. Arterial air embolism to the brain or heart may be the most common cause of immediate death from primary blast injury or of death at the moment when positive pressure ventilation is initiated.
Initially, treat all children who have potential pulmonary primary blast injury with 100% oxygen.
Casualties who present with asymmetrically decreased air entry and evidence of shock call for an immediate attempt at needle thoracentesis to decompress a potential tension pneumothorax.
This life-threatening condition may be caused by any combination of primary, secondary, tertiary, or miscellaneous blast injuries.
Acute respiratory distress syndrome (ARDS) may develop within 24 to 48 hours of injury.
Head Injuries
Blast fatalities associated with head injuries are basically related to subarachnoid and subdural hemorrhages. Among survivors, significant traumatic brain injuries are usually easily identified. Remember, however, that mild traumatic brain injuries are common and may be overlooked. Other injuries may also serve to distract the medical provider, making the diagnosis of subtle neurologic findings more difficult. Take into consideration subtle signs and symptoms of potential mild traumatic brain injury, such as memory problems, headaches, fainting, uneven gait, blurred vision, irritability, and confusion.
Abdominal Injuries
Primary intestinal blast injury is uncommon and depends on exposure to a very high air pressure. Injuries may include intestinal petechiae, hemorrhages, large intramural hematomas, intestinal laceration, or bowel perforation. The colon, where gas accumulates, is the most common site of injury. Ruptures may occur acutely or several days later due to stretching, ischemia, and subsequent weakening of the bowel wall. A tension pneumoperitoneum may also occur. Mesenteric, retroperitoneal, or scrotal hemorrhages are other potential injuries.
Eye Injuries
Up to 10% of all blast survivors have eye injuries. Perforations from high velocity projectiles present as penetrating trauma. Assess patients for altered vision, eye pain, foreign body sensation, decreased visual acuity, hyphema, or lacerations.
Ear Injuries
Blast injuries to the ear can be easily overlooked. Tympanic membrane perforation is the most common injury; however, injuries to the ossicular chain occur in 33% of cases of ear trauma. Inner-ear sensoroneural hearing loss may also occur. Blast related eardrum perforation may have local consequences, including infection, tinnitus, temporary or permanent hearing loss, and vertigo. Such patients need follow-up by otorhinolaryngologist.
Other Injuries
Other injuries associated with blast trauma include compartment syndrome, rhabdomyolysis, acute renal failure, severe burns, and inhalation of toxins. If the explosion occurred in an enclosed space or was accompanied by fire, tests for carboxyhemoglobin and electrolytes, as well as assessment of acid/base status should be performed. Elevated lactate levels are seen in cyanide toxicity.
Crush Injuries
Building collapse is a common disaster, particularly in earthquake situations. The collapse of a multistory building may cause crush injury in up to 40% of the extricated survivors. Crush injury should be suspected in any individual who has either had compression of parts of his/her body or has lain immobile on a hard surface for hours. In the Kobe, japan earthquake of 1995, among the 372 patients with crush syndrome, the mortality rate was about twice that of other trauma patients. It is important to note that the crush injury patients with associated injuries such as abdominal injury or extremity fracture had increased mortality rates (50% and 17.2%, respectively). Little information exists on children with crush injuries, but it appears that children have more recoverable renal function than adults. According to epidemiologic studies following the 1999 earthquake in Marmara, Turkey, infants seemed relatively immune to severe acute renal failure. Up to 20% of the cases of musculoskeletal trauma in Turkey occurred in people <18 years of age with the following injury patterns: ankle (30%), thigh (28.6%), head (23.8%), and forearm (7%). Many of these had crush syndrome in addition to their extremity injuries. Surgical amputations and multiple fasciotomies were performed on 12.6% of this pediatric population. Acute renal insufficiency occurred in 27% of these children; however, only 19% of earthquake victims needed dialysis, compared to 93% of adult victims that required hemodialysis (Sarisozen et Durak, 2003). Modern disaster plans need to anticipate high incidence of crush injury and be proactive in providing intravenous fluids in the critical hours following extrication, and even prior to extrication when possible.
Even short periods of entrapment can cause muscle compression injuries that may result in a crush syndrome, also known as traumatic rhabdomyolysis (Box 10). Crush syndrome is a severe systemic manifestation of trauma and ischemia involving soft tissues, mainly skeletal muscle, due to prolonged severe crushing. It leads to increased permeability of the cell membrane to sodium, water, and extracellular calcium and to the release of potassium, enzymes, and myoglobin from within cells. Cells begin to swell and intracellular calcium increase, thus disrupting cellular functioning and mitochondrial respiration, which all leads to myocytic death and can lead to compartment syndrome. Ischemic renal dysfunction secondary to hypotension and diminished renal perfusion results in acute tubular necrosis and uremia (Better OS et al, 2003; Ashkenazi et al, 2005).
BOX 10: Crush syndrome diagnostic criteria
- Muscle mass involvement
- Prolonged compression (usually 4–6 h, but possibly <1 h)
- Local circulation involvement
Gonzalez D. Crush syndrome. Critical Care Medicine 2005;33-1
Crush syndrome/traumatic rhabdomyolysis results from muscle reperfusion with subsequent secondary systemic effects. The destruction of muscle tissue and the influx of myoglobin, potassium, and phosphorus into the circulation results in the classic picture of traumatic rhabdomyolysis. The syndrome is characterized by hypovolemic shock and hyperkalemia. It is crucial to initiate volume expansion as soon as possible. Crush syndrome can result in several potential medical conditions that can be associated with significant morbidity or mortality (Box 11).
BOX 11: Clinical entities associated with crush syndrome
- Extreme hypovolemic shock
- Hyperkalemia
- Hypocalcemia
- Metabolic acidosis
- Acute myoglobinuric renal failure
- Compartment syndrome
Patients have classically been described as presenting with muscle weakness, malaise, and fever and commonly have other injuries such as pelvic and limb fractures, as well as abdominal injuries. The real danger lies in the cardiovascular effects resulting from electrolyte imbalance and renal failure. Look for the physical presence of skin trauma or local signs of compression (erythema, ecchymosis, abrasion, etc.) on the muscle mass. The absence of a pulse or a weak pulse to the distal limbs may be an indicator of muscle swelling or compromised circulation. Continued assessment may demonstrate a pale, cool, tense, edematous and diaphoretic limb with progressive loss of sensation, movement, and vascular circulation. Perform a lab evaluation for urine myoglobin, serum creatine phosphokinase, and serum electrolytes whenever possible. If nothing else an EKG should be done to look for STsegment changes resulting from hyperkalemia.
Key aspects to therapy are volume expansion through intravenous fluid resuscitation, ensuring alkalinized diuresis, and early detection of metabolic abnormalities. Initiate normal saline 20 mL/kg bolus at the scene of disaster, before or after extrication. Actually, normal saline or LR should be used with the addition of Nabicarb. Once the patient is hemodynamically stable, switch intravenous fluids to 50% normal saline with 40 mEq sodium bicarbonate for urine alkalinization with a goal infusion of 20ml/kg/hour in adults and children with a goal urine output of at least 2 cc/kg/hour (Ashkenazi et al, 2005). A urine pH between 6 and 7 has been identified as a reasonable goal (Better, 1990). The addition of bicarbonate avoids precipitation of toxic myoglobin metabolites in nephrons, improves acidosis, and facilitates a drop in serum K levels (Levinsky, Harrison’s Principals of Internal Medicine).
Diuresis can be forced with the use of either furosemide or mannitol. Furosemide is believed to help by causing renal vasodilatation, decreased renal oxygen demands, and increased renal intratubular flow. Mannitol works as an osmotic diuretic and volume expander. The goal of diuresis is to increase the elimination of myoglobin by the kidney and prevent deposition which leads to renal failure. It has been suggested that if rehydration fluids are not successful in achieving diuresis within 4 hours, then mannitol should be administered. The maximal daily dose of mannitol is 2 g/kg/day (not to exceed 200 g). Mannitol should not be used in patients with heart failure or established anuric renal failure. Administer analgesics, such as opiates or ketamine. If diuresis can not be achieved with lasix and manitol, given adequate hydration, then preparation for dyalisis is needed.
abnormalities.
One of the leading causes of death from crush injuries is severe hyperkalemia (serum potassium >7.0 mEq/L). Hyperkalemia generates electrocardiographic (ECG) disturbances, such as peaked Twaves, loss of P-waves, and widening of the QRS complex, which if not treated can progress to the deadly torsades de points. Treat symptomatic hyperkalemia or hyperkalemia with ECG disturbances with calcium chloride 10% (0.2 mL/kg IV) or calcium gluconate 10% (0.5-1 mL/kg IV) to stabilize the cardiac membrane. Of note, intravenous calcium may be ineffective as a treatment for hyperkalemia if given to a patient with hyperphosphatemia.
Additional treatment measures include mobilization of potassium into the intra-cellular space by plasma alkalinization (sodium bicarbonate 1 mEq/kg IV) or glucose administration (0.5-1 g/kg, 25% dextrose in water) plus insulin (0. 1 units/kg IV); albuterol aerosol; or kayexalate (sodium polystyrene sulfonate) 1 mg/kg orally or by rectal route. In extreme cases, hemodialysis may be needed (Cronan and Norman, 2000; Gaffar, 2003).
Hypocalcemia is defined as a calcium concentration <9 mg/dL. Clinical presentation includes weakness, paresthesias, and irritability, with ECG findings of prolonged QT interval, bradycardia and arrythmias. Treatment focuses on calcium administration, with continued ECG monitoring and calcium serum level determinations.
Intensive care support often is required for crush syndrome complications. Patients with anuria or oliguria are likely to require hemofiltration or dialysis. Aggressive treatment is necessary to decrease mortality and morbidity. Treatment during the acute phase of the rhabdomyolysis is aimed at maintaining adequate circulating volume and sufficient diuresis to prevent renal, cardiac, and pulmonary complications.
It is possible that crushed victims can progress to compartment syndrome, a situation that occurs when there is an increased pressure in a muscle compartment. This can lead to ischemia with eventual muscle necrosis and nerve damage (palsies). The anterior compartment of the lower leg is the most commonly affected; as there are four susceptible compartments in this commonly injured location. In severe trauma the compartment integrity may actually be disrupted, preventing high intra-compartment pressures from being reached. Clinicians should look for increasing and severe pain, especially pain associated with passive extension of the compartment.
The compartment syndrome examination is geared toward the classic description of the "five Ps":
- Pain out of proportion for the injury or pain to passive movement of the fingers or toes
- Pallor of the extremity
- Paralysis
- Paresthesias
- No pulse or reduced pulse
Confirmation of elevated pressures may be obtained by direct measurement of the compartment. Definitive treatment in the presence of a compartment syndrome is surgical release of the compartment connective tissue, i.e., fasciotomy.
Always consider compartment syndrome when the diagnosis of crush syndrome is suspected.
The development of a compartment syndrome in crush injury is due to the uptake of fluid into damaged muscle tissue that forcedly remains within a restricted compartment. Once compartment pressure exceeds capillary perfusion pressure at about 30 to 40 mm Hg, the tissue inside the compartment becomes ischemic and compartment syndrome develops. Although the traditional treatment of the compartment syndrome is fasciotomy, some evidence indicates that initial treatment with mannitol can also decompress a compartment syndrome, avoiding the need for surgery (Better, 1999).
6. Summary
The prospect of facing a community-wide disaster is daunting even to well-prepared hospitals. No hospital or other organization could be expected to perform effectively during such an event without previous training and practice. Conversely, the amount of relevant training and practice a medical team or facility has had can reflect substantially on its ability to perform well during a crisis.
The potential transfer of a large number of injured or traumatized children requires advance planning. Prior written transfer arrangements with other hospitals should be secured when anticipating mass disaster situations.
Several factors must be considered when preparing to transfer patients to other facilities. The most important is that they are stable for transport. The medical team must also ensure that the airway has been secured (remembering that bag-mask ventilation is preferable whenever possible), that breathing is not compromised by an untreated pneumothorax or hemothorax, and that circulation issues have been addressed and controlled.
Essential interventions after a disaster include systematic sorting of injured people
into different categories (triage), management of trauma by stabilization of the injured individuals, and familiarity with the patterns of the most common lesions.
7. Suggested Reading
- Aggerwal SJ, Diller KR, Blake GK, et al. Burn-induced alterations in vasoactive function of the peripheral cutaneous microcirculation. J Burn Care Rehabil 1994;15:1-12.
- American College of Surgeons, Committee on Trauma. Advanced Trauma Life Support. 6th ed.,1997.
- Better O. The crush syndrome revisited (1940-1990). Nephron 1990;55:97-103.
- Better O. Rescue and salvage of casualties suffering from the crush syndrome after mass disasters. Military Medicine. 1999;164:366-369.
- Cartotto R, Ellis S, Smith T. Use of high-frequency oscillatory ventilation in burn patients. Crit Care Med 2005;33(3):175-181.
- Cronan K, Norman ME. Renal and electrolyte emergencies. In: Fleisher GR, Ludwig S, eds. Textbook of Pediatric Emergency Medicine. 4th ed. Philadelphia, Pa: Lippincott Williams and Wilkins; 2000:820-822.
- Gaffar M. Diagnosis and treatment of hyperkalemia. Resid Staff Physician 2003;49:18-21
- Gausche M, et al. Effect of out-of-hospital pediatric endotracheal intubation on survival and neurologic outcome. JAMA 2000;283:783-790.
- Gonzalez D. Crush syndrome. Crit Care Med 2005;33:1.
- Kagan RJ, Warden GD. Care of minor burn injuries: an analysis of burn clinic and emergency room charges. J Burn Care Rehabil 2001;22:337-40.
- Kassis K, Grady M. Trauma and burns in Johns Hopkins. In: Gunn VL. Nechyba C, eds. The Harriet Lane Handbook: A Manual for Pediatric House Officers. 16th ed. St. Louis, Mo: Mosby; 2002:79-94.
- Nichols D, et al. Golden Hour: The Handbook of Advanced Pediatric Life Support. 2nd
edition. St. Louis, Mo: Mosby; 1996. - Sheridan RL, Petras L, Basha G, et al. Planimetry study of the percent of body surface represented by the hand and palm: sizing irregular burns is more accurately done with the palm. J Burn Care Rehabil 1995;16:605-606.
- Sheridan RL. Burns. Crit Care Med 2002;3011 Suppl): S500-14.
- Schwartz SI, Shires GT, Frank CS. Principles of Surgery. 5th ed. New York. McGraw Hill; 1989.
- Thomas SJ, George CK, Herndon DN. Burns: Military Options and Tactical Solutions. J Trauma 2003;54(5):207-208.
- Wolf SE, Rose JK, Desai MH, Mileski JP, et al. Mortality determinants in massive pediatric burns: an analysis of 103 children with >80% TBSA burns (>70% full-thickness). Ann Surg 1997;225(5):554-569.
8. Case Resolution
Case 1.
This patient needs immediate treatment and transport. He has suffered injuries to the thorax, head, and lower extremities. Initial evaluation confirms respiratory distress and shock. Snoring is probably due to airway obstruction by soft tissue, blood, or broken teeth. Adequate positioning of the airway and suctioning may alleviate the problem. Stabilize the cervical spine immediately.
The patient presents with hypoxia, with altered influx of air due to lung contusion or
tension pneumothorax.
If the child does not respond to positive pressure ventilation and 100% oxygen, needle decompression of the right hemithorax would be indicated. Also consider endotracheal intubation if oxygenation does not improve with the less invasive airway intervention.
Stabilize the femur by splinting. On the way to the hospital, administer IV fluids for
intravascular volume expansion. Quickly refer the patient to a center with pediatric care specialized units.
Case 2.
The girl appears to have suffered an isolated head injury with cranioencephalic trauma. Her rapidly deteriorating condition suggests intracranial expansive hematoma, a potentially deadly condition. As in any traumatic brain injury, consider the risk of a spinal-associated lesion. Stabilize the dorsal spine. It is important to be alert to possible vomiting. Administration of 100% oxygen and immediate transport to a center with a neurosurgical pediatric unit by plane if there is no such facility in the area are warranted.
On the way to the hospital, place an IV access to administer medication. This is an emergency, and enabling this patient to go immediately into the operating room may make the difference between life and death.
9. Module Review
Section I - Response to a Disaster
- What aspects should a plan for a disaster include?
- How is the rescue personnel organized?
- What specific equipment is needed for the management of children?
- What are the major dangers in the disaster scene?
- What priorities should be considered during transport of a traumatized child?
- What is the importance of having a standardized system for the classification of patients?
Section II - Pediatric Trauma Assessment
- When managing generalized trauma, what specific differences should be considered with children?
- What are the steps in the assessment of pediatric trauma?
- What precautions should be taken when managing a child’s airway?
- What are the most common traumatic injuries in children?
- How are thoracic lesions managed in children?
Section III - Disaster Specific Traumatic Injuries
- How are airways managed in patients with severe burns?
- How are burns classified?
- What is the initial care in burn patients?
- What are blast-related lesions?
- How is crush syndrome recognized and treated?
10. Appendix
CARVAJAL-GAVLESTON FORMULA
- First 24 hours:
- 5,000 mL x BBSA (m2) + 2,000 mL x TBSA (m2)*
- Ringer's lactate (half in the first 8 hours and the rest in the following 16 hours). No colloid should be given.
- Second 24 hours:
- 3,750 mL x BBSA (m2) + 1,500 mL x TBSA (m2) of dextrose solutions with electrolytes (based on patient's electrolytic anomalies)
*BBSA (burned body surface area): Formula: TBSA x %/100
**TBSA (total body surface area): Formula: (W (kg) x H (cm)/3600)
Notes:
Colloids are recommended at least 12-24 hours after the burn, using albumin poor in salt 1 g/kg/day divided in 3 doses (this aims at maintaining albumin levels above 2.4 g/dL).
If the patient develops myoglobinuria or hemoglobinuria (electrical burns, for example), take the following steps:
- increase fluids administered to achieve a urine output of 3-5 ml/kg/hour
- add bicarbonate to solutions
- if urine output does not improve, add mannitol to therapy