Text size
Line height
Text spacing
Pediatric head injuries are among the most common pediatric traumatic lesions. In general, children have a thinner and more flexible skull that transfers force of trauma to the brain more intensely than in adults. Anatomically, younger children have a disproportionately larger head and weaker neck muscles than adults. When these children are involved in a trauma event, they tend to "lead with their heads." When a child presents with a significant brain injury, also known as a traumatic brain injury (TBI), consider oxygen delivery to the brain and cerebral perfusion pressure (CPP).
CPP is the difference between the mean arterial pressure and the intracranial pressure. It is important to maintain a good mean arterial pressure and to perform measures that decrease the intracranial pressure. Some measures, however, can be performed only in the intensive care setting.
When the intracranial pressure rises significantly, vital signs can be altered. Cushing's triad consists of hypertension, bradycardia, and irregular breathing pattern. In children, bradycardia is typically the first manifestation and may serve as a sign of impending brain herniation.
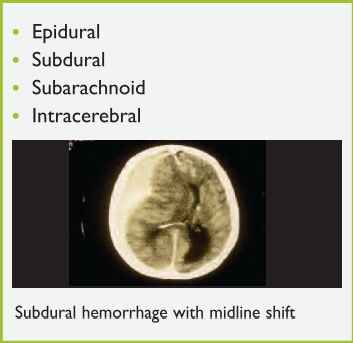
TBI can be classified as either primary or secondary. Primary brain injuries are those produced during trauma and may include brain contusion, diffuse axonal injury, or intracranial hemorrhage (Figure 7).
Secondary brain injuries include those that appear later as a result of metabolic effects, such as cerebral ischemia and cerebral edema. These injuries are usually seen hours to days after the traumatic event and can be minimized with proper medical care.
The management of a child that presents with a TBI begins with the ABC (airway, breathing, circulation) approach. The airway needs to be maintained with cervical spine precautions. All children should receive 100% oxygen, and intubation should be considered for GCS score <8, or for patients in whom it is not possible to maintain a stable airway. Ventilation should be assisted to maintain a PCO2 of 35 to 40 mm Hg. If there are clinical signs of brain herniation or neurologic deterioration, a lower PCO2 may be warranted.
Circulation issues include maintaining the mean arterial pressure and avoiding hypotension. Intravenous access needs to be established and either normal saline, lactated Ringer's solution, or packed red blood cells can be given. If hypotension is still present after volume expansion, cardiovascular vasopressor medication may be needed. Once the child is euvolemic, intravenous fluids can be administered at a maintenance rate.
Trauma laboratory studies and radiographs can be obtained as needed and may include serum electrolytes, glucose, complete blood count (CBC), partial thromboplastin time (PTT), prothrombin time (PT), and international normalized ratio (INR) (Significant TBI can cause coagulation alterations.). Maintain the head in a neutral position with a rigid cervical collar in place.
Provide short-term sedation and analgesia, such as midazolam (0.1 mg/kg) and fentanyl (1-2 mcg/kg) or thiopental. Thiopental reduces cerebral oxygen consumption; however, it is a cardiac depressant and can cause vasodilation. If there are clinical signs of intracranial hypertension, such as an unequal pupil dilation, abnormal posturing, or Cushing's triad, consider additional therapeutic measures including deep sedation, mannitol (0.51 g/kg), and hyperventilation (at PCO2 of 25-30 mm Hg) until clinical signs improve. Hyperventilation should be limited to serious injuries without adequate response to other interventions. Finally, consider placement of a Foley catheter and a nasogastric or oral-gastric tube in patients with severe post-traumatic brain injuries.