Text size
Line height
Text spacing
First, assume that the health care facility, wherever its location, will need to function alone until outside help arrives. It is, therefore, important to have a notification system to call in extra personnel.
It is always essential to use a triage (injured patient classification) system and to prepare adequate treatment areas to handle the influx of patients. Free up operating rooms and intensive care beds and carefully check on all available supplies (blood, medications, communication equipment). Always consider that decontamination procedures may need to be implemented as indicated. It is also necessary to ensure security in the emergency setting and to start transferring the injured people according to the priorities established through the classification process and the available resources. A public information center will be needed to distribute information to media and families. Annual drills help familiarize the staff with the disaster plans, as well as provide feedback to finetune the plans.
Having a list of available personnel and appropriate means to contact them is a critical preparatory step in the face of a disaster. Arrange a central communication system that can activate a call-up roster to ensure the timely arrival of this help.
Once the personnel are at the medical facility, it becomes important to organize this labor force and provide job descriptions. A military model has been adapted to the hospital setting and is referred to as the Hospital Incident Command System (HICS). HICS has become the standard for health care disaster response and offers predictable management schemes, flexible organizational charts, prioritized response check-list, accountability of position function, and common language when communicating with outside groups.
Your health care unit is sent to a neighborhood to see a child who has suffered a fall. You find an 8-year-old boy lying on the grass near a big tree. An adolescent tells you that she saw him fall from the tree when he was at a height of about 30 feet. Nobody has moved him.
Initial assessment shows that the boy is responding only to painful stimuli. Breathing is superficial with audible snoring. The skin is pale, with mild cyanosis. Respiratory rate is 12 breaths per minute; heart rate is 130 beats per minute.
The skin is cold, radial pulse is weak, and capillary refill is >3 seconds. Pupils are equally dilated and are reactive to light. Air influx cannot be detected through auscultation in the right hemithorax and is diminished in the left. Oxygen saturation is 82%.
He has broken teeth and a swollen nose, with moderate hemorrhage. The abdomen is stiff on palpation. The right leg is swollen, with evident deformity to the femur.
Specific equipment must be available in disaster emergency situations involving children. Box 1 displays a list of recommended equipment.
BOX 1: Recommended equipment for pediatric emergencies in disaster situations
Airway Management
Intravascular Access or Fluid Management
Miscellaneous
Monitoring Equipment
Among the recommended equipment, elements for proper airway management in children are crucial. A major challenge of any disaster response is gathering, organizing, and moving supplies to the affected area. Resource management within the hospital and other facilities or agencies may prove to be a decisive factor in whether a mass casualty event can be handled or not.
A very important aspect during a disaster situation is the ability to communicate, not only with others in the community but also among the medical personnel involved in responding to the situation. A coordinated response is needed in order to adequately handle a large influx of patients. Ideally, personal radios or cell phones should be available, so that the personnel involved in health care management communicate with each other and with the central command leader. The same applies to other areas (administration, security, maintenance).
Most physicians are not trained in onscene rescue efforts. In general, local police, firefighters, and hazmat teams are the best to initially approach and control a disaster scene. However, in confined spaces, triage may need to be set up in the field and this may put the health care providers close to the disaster location.
Risks at the actual disaster scene vary according to the nature of the disaster. These include: structural instability and further collapse, fires, carbon monoxide, cyanide, dirty bombs, contamination with biologic material, and infectious agents. Other potential hazards in confined spaces include: poor air quality, airborne pollutants, toxic gases, an explosive/flammable atmosphere, and insufficient oxygen concentration (Box 2).
BOX 2: Risks at a scene of a disaster
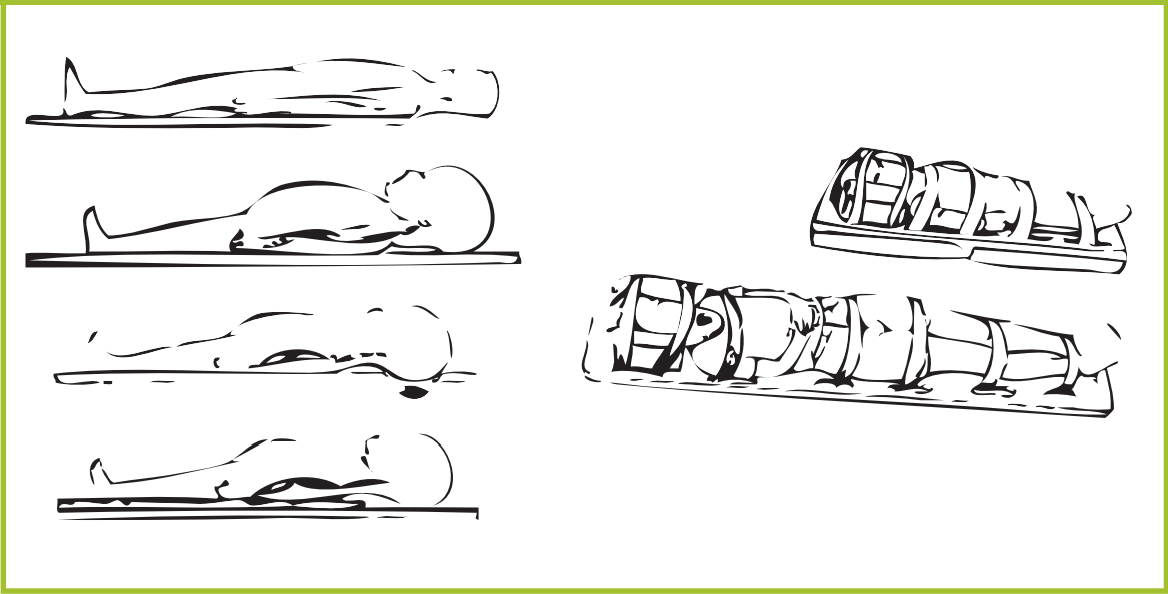
Ideally, patients will be promptly transported to a local medical clinic or hospital. The initial response at the scene of a large disaster, once the patient has been rescued, includes airway support, spine immobilization, and oxygen delivery. The increased neck flexion that occurs from the large head of small children on a backboard can be addressed with either a scooped-out head area on the backboard or with a small roll of cloth placed under the shoulders to elevate the trunk (Figure 1). Immobilization on a backboard is primarily expected to protect the spine during transport and facilitate transport. It is important to get the child off the backboard within a couple of hours.
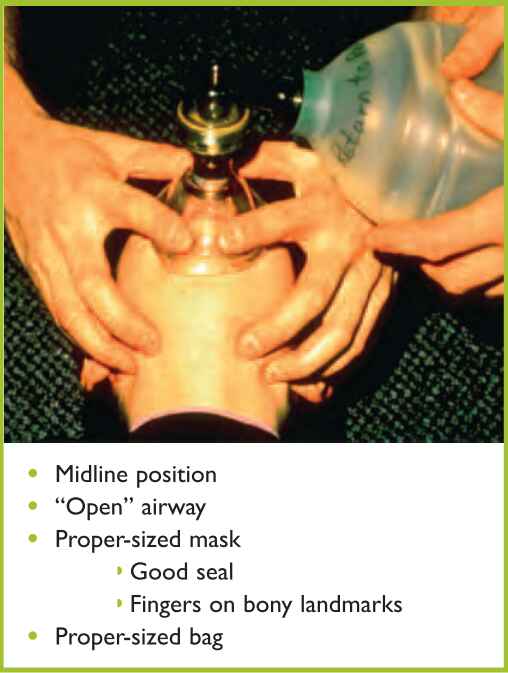
Keeping the airway open during transport of the traumatized child is a top priority. Airway support can be adequately maintained with bag-valve-mask ventilation (BVM). Intubation in children prior to transport is not necessary and has not been shown to improve outcome. In fact, endotracheal intubation can lead to delayed transport and increased morbidity due to improper tube placement or possible dislodgement of the tube during transport. A large study in children compared endotracheal intubation versus BVM in the pre-hospital setting. This study included 830 patients below age 13, randomly assigned to BVM or endotracheal intubation. Results showed that there was no advantage in placing an endotracheal tube (ETT) prior to transport to a hospital (Gausche et al., 2000). This adds to the risks that may arise from improper ETT placement. Therefore, proper BVM technique remains one of the most important skills to teach and review with local first responders to a disaster situation (Figure 2).
Injured individuals with high morbidity or mortality risk should be promptly transported. The highest level of pediatric health care is needed for falls, fires, explosions, blunt injuries, and penetrating injuries (Box 3).
BOX 3: High-risk pediatric injuries