Text size
Line height
Text spacing
These activities include the procedures needed to organize the disaster zone. The alert
given by any observer sets the process into motion. Define exactly the location of the disaster event, the time of its occurrence, its type, the estimated number of victims, the risks, and the population threatened by these risks.
The initial assessment will establish what resources will be mobilized at the site of the disaster (Figure 3).
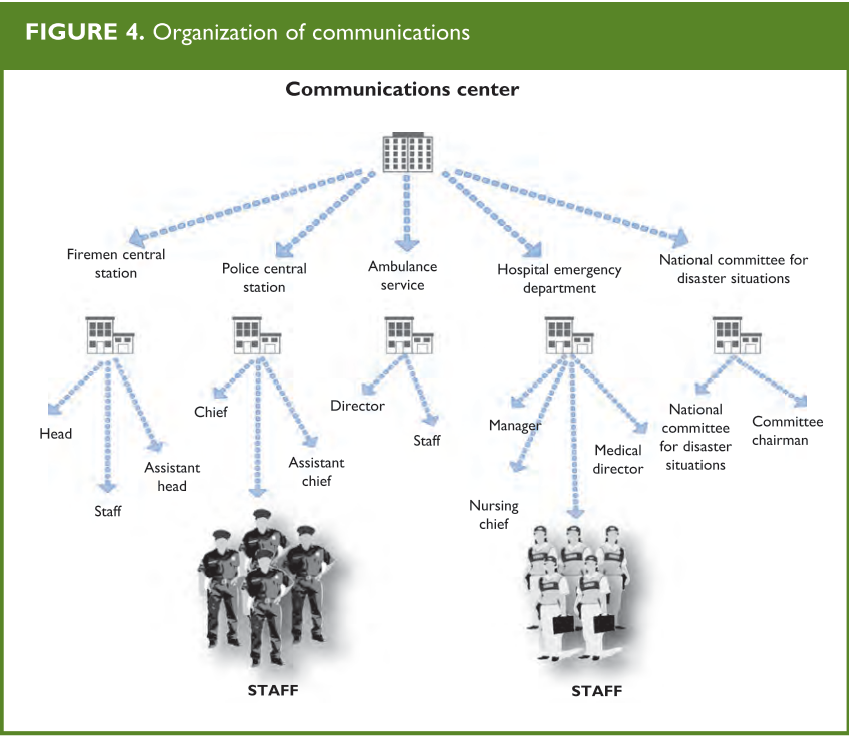
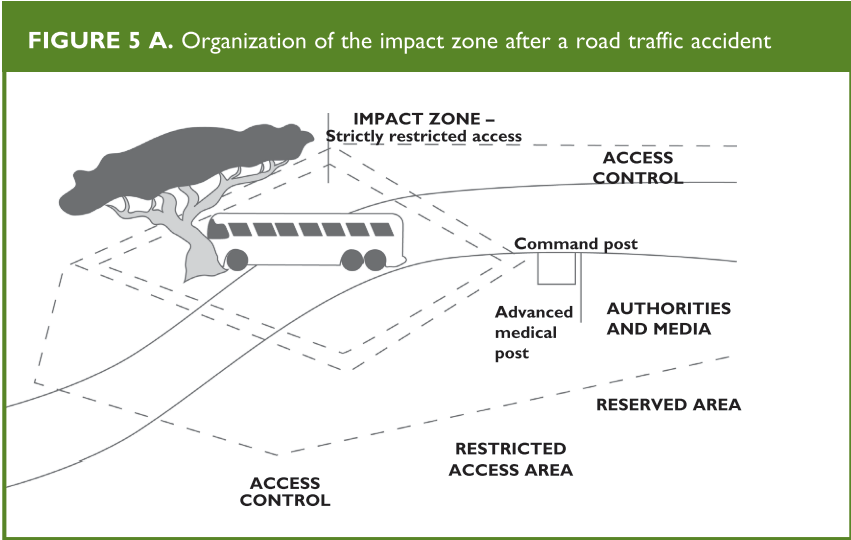
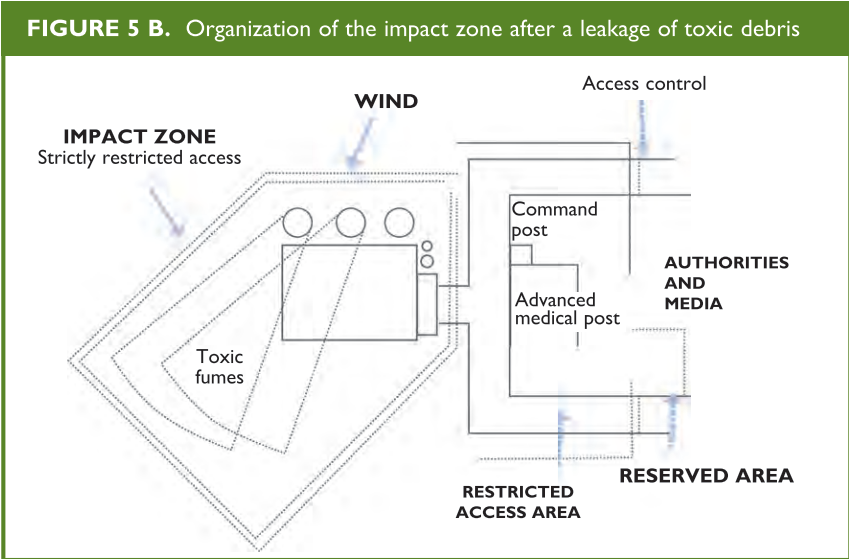
The initial evaluation unit identifies the zones to be set up at the incident site:
(Figures 4 and 5 A and B)
Appendix B, page 39, displays a number of function cards that define in detail the basic
activities of the professionals involved in the coordination and the care of victims in a MCI.
From: Establishing a Mass Casualty Management System, Washington D.C., 1996
Rescue activities during a disaster should include measures to guarantee the safety of the victims, the members of the rescue units, and the general population.
When a disaster occurs, both landline telephones and cell phones could be overburdened.
The communication method of choice for emergency organizations utilize ultra-high frequency (UHF) and very high frequency (VHF) waves. The former are used for communications within the area of the event, and the latter provided from the site to the Incident Command and from there to intervening agencies and the nearest hospital.
for communications with strategic centers for purposes of coordination or transportation. Patient referral information should be provided from the site to the Incident Command and from there to intervening agencies and the nearest hospital. Essential information to be collected includes:
From: Establishing a Mass Casualty Management System, Washington D.C., 1996.
Search and rescue activities should be performed by individuals with specific capabilities including firefighters and specialized rescue units. Before allowing these individuals to enter the disaster area, verify whether they need special clothing or breathing equipment to protect them from environmental risks.
Once the search and rescue units have located the victims, they must take them to a risk-free casualty collecting point to be assessed (field triage).
After this initial triage, the victims receive first aid according to their status. When the number of victims or the distance from the place of the incident prevents the direct transportation of all victims to hospitals, an advanced medical post may be established adjacent to, but outside of, the impact zone.
From: Establishing a Mass Casualty Management System, Washington D.C., 1996
Prior to the advanced medical post, all victims are medically triaged (see “Triage: Rationale” below), to identify those who require immediate care.
Following triage classification, victims are referred to the adjacent treatment areas within the advanced medical post where they are stabilized. Stabilization procedures may include advanced airway management fluid therapy to maintain circulation and treat shock, control of hemorrhage, and analgesics. Document the therapies given in the patient’s evacuation report that accompanies the patient to the hospital. In summary, goals of the advanced medical post are to stabilize patients, reassess their condition (retriage), and organize their transportation to the appropriate hospitals. All these tasks have been summarized as the 3 Ts principle: typifying (classifying), treating, and transporting.
Ideally, the advanced medical post should be staffed with trained emergency medicine physicians and nurses; additional physicians such as surgeons and anesthesiologists can be added if available and needed.
Triage is a system that allows establishing priorities for care and transporting in order to save as many lives as possible. It is performed during the rescue phase, and uses priority criteria for the care of patients, distinguishing those requiring immediate stabilization and transport from those who can wait. In a more detailed analysis, triage also allows for identifying patients who need emergency surgery. The primary triage in a MCI consists of a quick evaluation so that all the victims can be examined in a short period of time and decisions can be made regarding treatment priorities.
Once the victims are brought to the collection point, the staff responsible for triage must quickly assess each and every victim, and refrain from providing treatment other than hemorrhage control and brief airway repositioning. Specific algorithms, such as the START (Simple Triage and Rapid Treatment, Figure 6) have been used to streamline this process using a color-coding system. START triage evaluates for respirations, pulse/perfusion, and mental status. All patients are triaged first prior to initial medical interventions. During this evaluation, each victim is identified with a specific color-coded tag, tape or marker to indicate the level of medical urgency needed. Primary triage is based on the premise that all the victims are equally important, regardless of age, gender, profession, or any other factor. Decisions are made exclusively based on the victim’s clinical condition. Patients are classified according to severity as green (uninjured or minimally injured), yellow (moderately injured or urgent), Red (severely injured or emergent), and Black (deceased). Field triage is performed on three levels:
Classifies the victims to identify those who need to be taken immediately to the advanced medical post. First aid providers or medical emergency technicians usually do this on-site triage. When the technicians do not have extensive experience in triage, consider having them classify the victims in the “yellow” and “red” groups together as one. Using this approach, the percentage of incorrect classifications declines significantly. In addition, this simplified classification results in a reduction of the time required for the initial evaluation.
Determines the required level of care. An emergency physician, anesthesiologist, or surgeon should be in charge of this type of triage.
Red: Immediate stabilization is required.
This applies to victims who have:
Stabilize these patients so they can receive further care. After stabilization, reclassify.
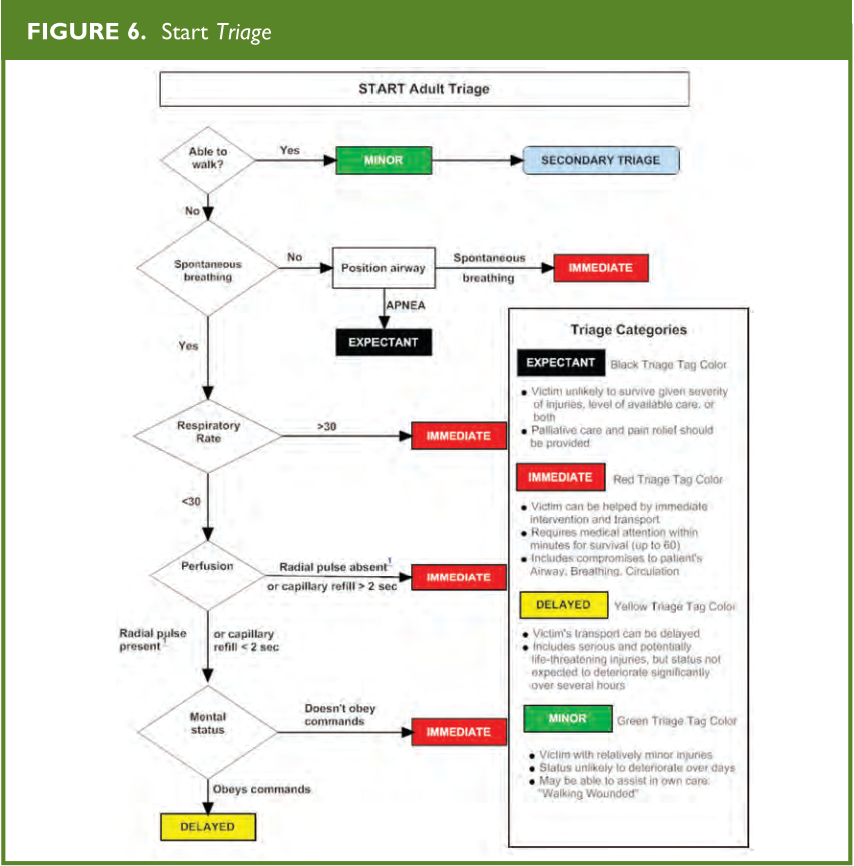
From: Radiology Emergency Medical Management, https://www.remm.nlm.gov/StartAdultTriageAlgorithm.pdf; adapted from original: Lou Romig, MD
Yellow: Delayed treatment may be appropriate. Monitor closely, insert a line if uncertain about circulatory status, but defer care initially. This category includes victims who, despite not fulfilling the criteria for inclusion in the red group, have:
Green: These victims can wait or do not require treatment. This category includes those who are ambulatory and have:
After on-site care has been completed, transport victims who have been classified as yellow or red to a hospital. They should be re-triaged on arrival.
Black: Deceased.
Victims are reclassified in terms of their priority for transportation to the nearest hospital.
Red : These victims have the highest priority for transport, preferably with a specialized crew to a tertiary hospital because they require surgery for survival or organ-function preservation or need ICU services.
Yellow : These victims have the second highest priority for transport, which includes victims who are currently stable but may decompensate or require urgent but not emergent surgery.
Green : These victims may be discharged on-site, if possible, after being checked and reassured. Those with minor injuries should be treated or sent to a primary care facility if available.
Black : Transportation to the morgue.
The JumpStart triage system is a modified triage algorithm of START based on physiological criteria adapted to the normal range of pediatric values (Figure 7).
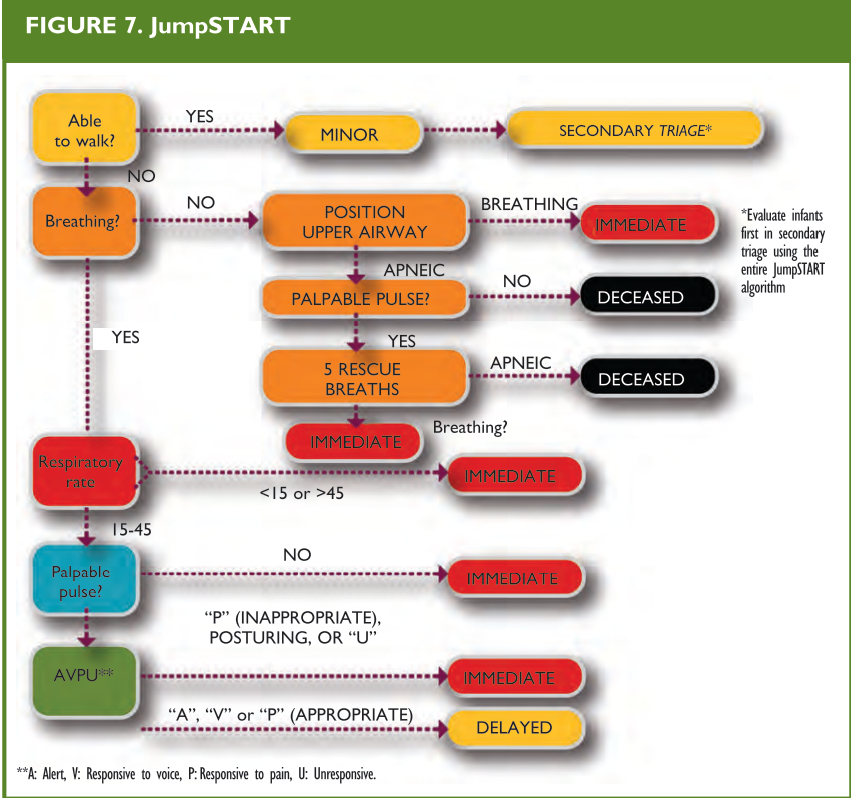
From: Romig LE. Disaster Management. In: APLS Course Manual. Jones & Bartlett Publishers, 2006.
Unlike the adult-based triage system, this system recognizes that an apneic child can still maintain a certain degree of perfusion before he/she develops an irreversible cardiac lesion secondary to anoxia. These children can survive if their respiratory function is sustained or restored, something that will not be identified by applying the START system (Figure 6), which does not include pulse palpation for patients whose apnea persists after the airway has been opened. Children who are not able to walk or are carried in arms by adults should always be categorized at the very least, as yellow.
Regardless of the triage system used, perform a careful secondary evaluation on all the victims on-site and then again at the emergency department. Triage is a dynamic process and continues until the patient arrives at a place where he/she is offered definitive evaluation and treatment.
There is a newly proposed national for mass casualty triage called SALT for both adults and children (see Appendix B). SALT stands for “Sort, Assess, Life-saving interventions, and Treatment.” This guideline was developed due to the multiple triage systems, many of which have been inadequately guideline validated. This guideline was developed by an interdisciplinary committee of the AMA, the American College of Surgeons, the American College of Emergency Physicians, the National Association of EMTs, and various other representative organizations.
Global sorting is the first step to address the “walking wounded”. Those who are able to walk are prioritized last; those who cannot follow a command or have an obvious life threat are prioritized first; and those who can follow a command but are unable to walk are prioritized second. The next step of this triage system is to make lifesaving interventions before assigning a patient to a triage category. Lifesaving interventions include control of major hemorrhage, opening the airway and providing 2 breaths for child
casualties, decompression of a tension pneumothorax, and use of autoinjector antidotes. Finally, triage categories are assigned to be Delayed, Immediate, or Expectant management based on breathing, peripheral pulses, respiratory distress, and hemorrhage control. This system of triage is different from the other systems in that there is a grey or “Expectant” category. This category means that the patient may have a life threatening injury, but current resources are not available to meet the demand. The “expectant” category of patients should be re-evaluated frequently as resources become available.
This system of triage does not assign “colors” to patients; therefore, it should not be confused with other triage systems. The SALT triage system is an attempt to take the best features of triage systems that have been tested. It is a different method of triage in that there is global sorting based on the ability to follow commands and walk, and a triage
category assignment based on response to life-saving interventions. Children would likely be over-triaged to the “assess 1st category,” as many will not be capable to follow commands due to developmental stage. This over-triage is probably inherent in pediatrics and can not be avoided. This SALT system of triage should be tested against the most commonly used form of pediatric triage: Jump START.