Planning and Triage in the Disaster Scenario
| Site: | Pediatric Pandemic Network Learn |
| Course: | Build Planning and Triage in the Disaster Scenario |
| Book: | Planning and Triage in the Disaster Scenario |
| Printed by: | Guest user |
| Date: | Sunday, June 14, 2026, 4:50 AM |
Table of contents
1. Overview
Welcome to this multimedia open access edition of Planning and Triage in the Disaster Scenario.
This content is available as a digital book in two formats:
1) Website, which you are currently reading. This format offers a mobile friendly multimedia experience with sharable links to chapters.
Use the chapter navigation to the left to navigate to different chapters in the book. Scroll through the links to select the chapter that interests you.
Use the yellow arrows that appear to select previous and next chapters.

2) Printable, which you can save as a PDF and open without an Internet connection.
2. Introduction
Authors:
Ciro Ugarte, MD
Jacobo A. Tieffenberg, MD, MS, MPH
Ribka Amsalu, MD, MSc
Lou E. Romig, MD, FAAP, FACEP
“Failure to plan is planning to fail.” This quote by Benjamin Franklin appropriately reflects the message of this module. Emergency preparedness planning is crucial to prevent or mitigate a disaster. As defined in Module 1, disasters occur when a natural or man-made event transforms a vulnerable human condition into a traumatic event causing needs to exceed the local capacity for response. Without adequate planning, the most common response to these types of incidents is confined to simply rescuing victims and transferring them promptly to a hospital facility (the “Scoop and Run” approach). This results in the transfer of the problem from the incident site to the hospital, overwhelming and disrupting the care capacity of the health facility.
Some events occur suddenly, with little or no warning. Others, such as flood and hurricanes, usually provide advanced warning or have a gradual onset that allows for additional preparations before the critical stage ensues. In any case, specific planning and preparedness are especially important to reduce the suffering caused by disasters, particularly for children. Children are among the most vulnerable populations in disasters because they have unique physiological, psychological, and developmental needs. Pediatricians and the local community have a special responsibility to assess how local, regional, and national preparedness plans and response systems will actually function to protect children. Failure to consider the needs of children in disaster planning, preparedness, and response at all levels potentially jeopardizes this vulnerable population. Pediatricians must advocate for the health, safety, and well-being of infants, children, adolescents, and young adults who cannot advocate for themselves. Increasing our understanding of how children were affected by past disasters will inform and strengthen our response.
The information provided in this module can assist in the design of an emergency preparedness plan that will increase coordination among the many disciplines involved in disaster response. Active participation of all relevant entities in plan development is crucial. Participation in planning among involved entities breaks down the silos that all too often isolate different disciplines, and promotes understanding and cooperation among them. The multidisciplinary, inclusive planning process is actually more important than the document itself. The planning process facilitates a collective understanding among all the key agencies and their personnel about the plan, which is indispensable for effective implementation of the plan when it is needed. Planning should include both short-term and more long-term ways of risk reduction from potential disasters, efforts to educate families and community organizations about preparedness, and methods of horizontal and vertical coordination involving multiple local entities as well as regional, national, and international assistance networks. Local planners need to have knowledge of the regional and national response systems and the means to coordinate local activities with these systems.
This module reviews the basic concepts for emergency planning and response preparedness, and discusses the various levels of planning which include the family, health professionals, community organizations, and health facilities. The final section of this module reviews how to organize community emergency services capable of responding to a mass casualty incident.
3. Local Emergency Plan
oBjectives
- Describe the components of the plan and the pediatricians’ role.
- Identify the risk factors that warrant consideration when planning for disasters.
- Know the basic requirements for the design and coordination of a local disaster plan.
The phases of disaster response include preparedness during which time there should be a risk assessment and mitigation; disaster response (the rescue mission) that involves warnings, evacuations, and saving lives during the immediate post disaster period; and the post disaster recovery period. Disaster management is part of the social system responsible for planning, organizing, directing, and controlling during all the phases of emergency management: Preparedness, Prevention, Response, and Recovery. The disaster plan should define the objectives, strategies, and activities, including a detailed chronology and a proposed budget.
The emergency plan will have different objectives depending on the phase. Disaster preparedness includes the design of the plan, the training and coordination of those who will execute it, and the availability of needed resources. The plan designed during this stage is generically named the response plan. A plan made for various adverse events is called an emergency or disaster plan, whereas a contingency plan is designed for a specific adverse event (e.g., tornado, flood, pandemic).
During the prevention phase, the ultimate goal is to avoid or mitigate the disaster, directing efforts aimed at reducing both the risk and the vulnerability of the population. In many events, damages will occur despite mitigation efforts, and this is defined as the remaining risk. To face these damages, the capacity for response must be improved through preparedness. If a disaster occurs, the plan will be implemented in order to provide medical and humanitarian assistance. The response phase consists of both implementation of previously derived preparedness plans, as well as any spontaneous actions felt to be needed even if not part of a formal plan. After the response phase, efforts will be directed towards repairing damaged services. This is known as the recovery phase. Reconstruction and recovery consists of restoring the goods and services back to pre-disaster levels if possible, and includes measures for future risk reduction.
Pediatricians and other clinicians that care for children need to be involved in all local committees that are considering risk management, preparedness, and response. They should be familiar with the plans that exist in their region so that they can work in coordination with other members of the response system. In summary, emergency planning includes all the activities and actions done preemptively in order to prevent, mitigate, respond to, and recover from the damages that disasters can cause. All stages of a disaster (described in Module 1) include elements of planning that are important for the pediatrician. These involve various social agents and are performed at different levels: the family, local community organizations, emergency services, community physicians, hospitals, government, and other agencies especially the local red cross and red crescent societies. The town or district public health offices are usually the convening agents for disaster preparedness and response planning.
This is not merely desk work. It involves obtaining and analyzing data, along with field visits and meetings with representatives from different institutions and the community. Preparation demands the active participation of the health-care sector and the community. These efforts should result in the production of operative and concise documents that clearly define the responsibilities of specific participants and the agreements reached among the participants. It is important to institute periodic drills to test the functionality of the system and the coordination among the different participants.
3.1. Risk Evaluation
A risk evaluation involves an analysis of threat and vulnerability. It considers the characteristics of potential threats to a community and determines how the community would be affected. Identify the possible natural events that threaten a particular community (e.g., earthquakes, torrential rains, volcanic eruptions, sliding soils, the overflow of rivers or lakes). In certain regions, the climatic events that endanger the population have a seasonal predisposition. Recognizing these climatic cycles can maximize preparedness before and during these periods. Do not disregard disasters caused by human actions. These include incidents in factories, chemical or fuel storage plants, intentional or accidental fires, incidents with radioactive or nuclear materials, armed conflicts, wars, or terrorism. In summary, risk evaluation involves identifying regions and communities that are most vulnerable to the threats under consideration, and describe the specific characteristics that make these communities susceptible to those threats.
3.2. The Community - Local Emergency Plan
Every community should develop its own emergency plan with the participation of the local institutions and agencies. Clearly define the responsibilities of each institution and methods of coordination and collaboration. Analyze the risks threatening the various sectors of the community and develop immediate interventions recognizing both geographic and climatic conditions for various regions. Obtain input from regional and national levels, involving national and regional health officers in the planning process.
3.3. Clinic and Hospital Emergency Planning Key Concepts
The emergency plan should fulfill four essential characteristics: it should be clear, concise, complete and widely disseminated.
- Clear: Make the wording simple and easy to understand, with no margin for doubt.
- Concise: It should be quick to read. The longer the plan, the less likely it will be read in its entirety and the more difficult it will be to update regularly and distribute.
- Complete: include all the necessary components for effective action, coordination, and reassessment.
- Disseminate: the plan should be widely disseminated to key stakeholders. It should also be summarized in a way that is visually attractive when displayed in office space and hospitals.
The plan describes the responsibilities of each participant, the risks involved, and the range of interventions. It is imperative to involve the organizations that will carry out the plan in the planning process itself. For a health-care agency, the emergency plan defines the objectives, the actions, and the organization of the hospital and its various departments with respect to the response activities and responsibilities of its staff members.
Additionally, the plan needs to be known by all entities involved. These elements are essential if the plan is to be executed in the pre-established manner.
3.4. Basic components of an emergency plan
Analysis of the situation
The analysis of the situation includes:
- a description of the threats, whether naturally occurring or due to human action.
- an analysis of the structural and nonstructural vulnerability of areas at risk in the community.
- an evaluation of how agencies would function to deliver needed services (operative capacity).
- the availability of resources, infrastructure, equipment, and critical supplies.
Assumptions
Identify the type or types of phenomena that should be addressed in the plan and describe the probable magnitude, the expected intensity at the site where the community is located, and the time period during which it is likely to occur. Determine the potential damages and the maximal demand for health services by establishing a relationship between the threat and the vulnerability.
Objectives and goals
The objectives and goals describe the expected outcomes from executing the emergency plan given the human, economic, and material resources that will realistically be available. One of the most frequent mistakes when preparing an emergency plan is to include nonexistent resources with the hope of obtaining them in the near future. Since it is usually impossible to obtain all the desired resources, establish priorities for the actions based on the population and geographical area to be served. The plan should include an outcome prediction that describes the measurable impact of carrying out the emergency plan.
Organization
Organize the various sectors and departments of the institution so that authority, lines of responsibility, and methods of coordination and communication for plan activation are clear and well-defined. Establish an emergency operations committee to oversee and coordinate response actions.
Roles and responsibilities
The assignment of roles and responsibilities is meant to answer the following questions:
- Who does what?
- When?
- How?
- With what?
It is important to have a clear command chain for communications with backup systems to mobile cellular service such as radios, megaphones, and mobile sound systems.
Communication and coordination
The communication instructions describe a calling or notification chain from a central point until all the necessary individuals have been contacted. Establish the means of communication to be used, indicating the radio band and frequency, telephone numbers, and rendezvous locations. Each location should have a team leader identified. Team leaders can do household counts to determine who might be missing and need to be rescued. Appendices to the plan include an updated directory of all the participants, a map of threats, vulnerable areas, or locations, as well as the population database, a health profile, health centers included in the network, a directory of basic services (e.g., water, electricity, telecommunications, security), assistance agencies, and an inventory of the available resources.
Training
Once the emergency plan has been developed, conduct training. Training should enable the participants to describe the situation, expected damages, roles and responsibilities, and means of coordination. This training should include simulation exercises. The participants will have to solve theoretical (tabletop) exercises once they have been assigned one of the roles and responsibilities contemplated in the plan. This exercise allows participants to assess their knowledge of the technical and organizational aspects of the emergency plan.
At a later stage, disaster drills can be organized and enacted. Organize disaster drills with prior notice, promoting the participation of the staff and key members of the community. Use the experience gained in the simulation drills to update the emergency response plan. Enacting unannounced simulated disasters without previously training participants usually causes frustration and has unwanted effects.
Resources
Analyze the activities included in the emergency plan to determine the resources required. This listing of resources is called the requisite analysis. Contrast the listed resources with those actually available and define the resources that are yet to be obtained. Gather the resources needed to carry out the emergency plan. Remember that the emergency plan must be based on reality. Otherwise, it will become a mere listing of wishful ideas.
See Box 1 for useful planning resources.
BOX 1: Resources for local emergency plan development in the United States
- Federal Emergency Management Agency (FEMA) – National Incident Management System (NIMS) publications at http://www.fema.gov/emergency/nims/
- Centers for Disease Control and Prevention - software planning model tools for governments at http://emergency.cdc.gov/cdcpreparedness/science/planningtools.asp
- Your state’s homeland security office, local government affairs office, or county government office, listings at http://www.fema.gov/about/contact/statedr.shtm
- Colorado’s Office of Homeland Security at http://www.colorado.gov/homelandsecurity
- The International Federation of the Red Cross and Red Crescent http://ifrc.org
3.5. Coordination of the local emergency plan
The response mechanisms will have specific characteristics depending on the size of each community and the particular risks that threaten it. The coordinators in hospitals, rescue services, and emergency medical services, as well as the participants processing the incoming information, should report to an incident commander who will direct the local emergency plan (Figure I). For incidences involving multiple jurisdictions and agencies, a unified command system may be established in which individuals designated by their jurisdictions work jointly to determine priorities, resource allocation, and strategies needed to execute the emergency plan. A coordinated emergency response between various levels of local, state, and federal government may be needed, in addition to non-governmental agencies providing humanitarian aid.
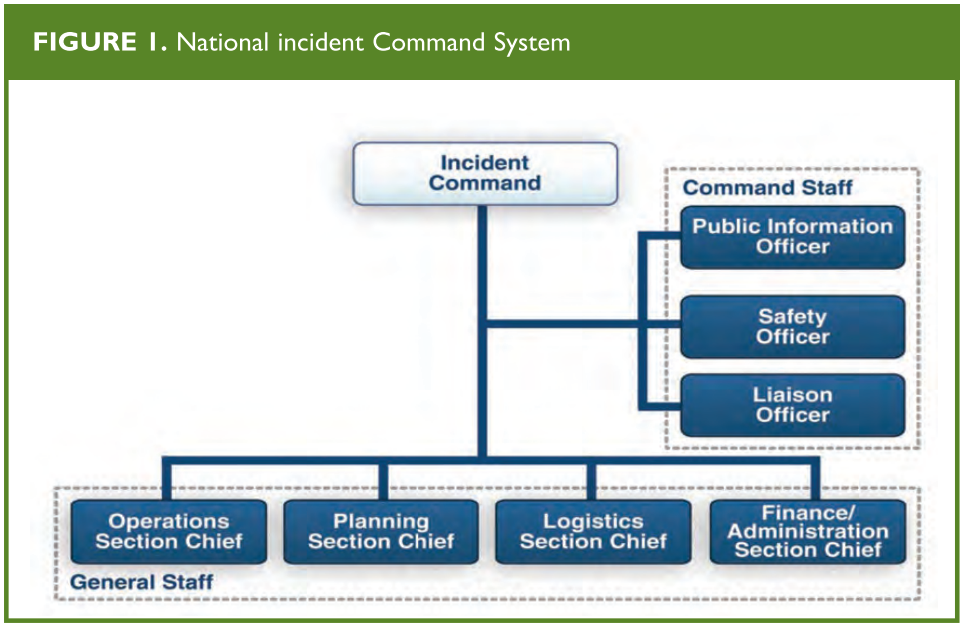
National Incident Command System (NIMS), U.S. Department of Homeland Security, Dec 2008
4. Planning Levels
objectives
- Identify the different levels of planning for disasters.
- Help families make a family emergency plan.
- Recognize the importance of one’s own planning, and the planning by other health-care professionals and health centers.
- Assist elementary and high schools in developing their own emergency plans and how they can integrate into the local community emergency plan.
- Identify the special needs that should be addressed in a disaster shelter.
- Describe the role of the Emergency Medical Services (EMS) in disaster response.
- Discuss state and federal emergency response plans.
Planning in the family
Pediatricians should prepare themselves for a disaster as well as provide the families of their patients with information about creating a family emergency plan. The questions below serve as a planning guide. Families need to understand that they have to be prepared to evacuate before the area becomes inaccessible by rescue services, and if they choose to stay, they might not be helped immediately.
Important questions that family plans must address are:
- What are the disasters most likely to occur in your community?
- Is your home, your children’s school, and your working place located in risk areas?
- How well-prepared is your home to face the most likely disaster?
- Can your family be notified with sufficient anticipation or should they be prepared in order to respond at any time?
- In the event of a disaster, can you locate and reunite your family members at a safe location?
All family members should know contact telephone numbers outside the affected area and know where community shelters will be located. It is also a good idea to have a pre-established meeting point outside the risk area when possible. Family should also know the location of the command center or evacuation site during typhoons, floods and other natural disasters.
What should you do when you or one of your family members need to leave the family because of healthcare or other related responsibilities during a disaster situation?
When professional duties (e.g., those of health-care professionals, policemen, firefighters, public officials) limit the ability to assist one’s own family, it is important to have a clear written plan that has been discussed and can be followed. An example would include having a retainer contract with a child care provider during a pandemic influenza outbreak.
Do any members of your family have special health needs that might be affected during a disaster?
Consider storing and periodically renewing medications and supplies needed by family members with special health-care needs for use in the event of a disaster. Consider having a small backup generator to keep a refrigerator operational to store medications when there is no electricity. Recognize that family members with special needs may require earlier evacuation to ensure a safe environment.
BOX 2. Supplies needed for 3 days of self-sufficiency
- Basic supplies
- Bottled drinking water (4 L/day/person)*
- Identity cards of all family members
- Well-equipped first aid kit and first aid manual
- Non-perishable food
- Matches
- Flashlight with batteries or hand-crank
- Extra clothing for protection from bad weather or outdoor stays
- Blankets or sleeping bags
- Money, including small change
- Insect repellent
- Personal hygiene products and sanitizer
- Various supplies for infants and small children
- Portable radio, cell phones (preferably with radio or walkie-talkies)
- Map of the city or region
- Frequently used medications and medical prescriptions.
- Some complementary supplies
- Manual can opener
- Garbage bags
- Two extra sets of home and car keys
- Elements to hold and transport pets (e.g., leashes, collars, kennels)
- Food and water for pets
- Extra glasses
*It is advisable to have enough drinking water for 1 week.
A list of supplies needed for 3 days of self-sufficiency for a high income country are shown in Box 2. This list should be modified for what is appropriate and feasible for low and middle income countries. A local specialist can add other useful supplies based on the local situation. Box 3 lists online resources for families.
BOX 3. Resources for families on the Internet
- American Red Cross Family Disaster Education Materials at http://www.redcross.org/
From: Romig LE. Disaster Management. In: APLS Course Manual. Jones & Bartlett Publishers, 2006.
A local specialist can add other useful supplies based on the local situation. Box 3 lists online resources for families.
4.1. Planning by the medical staff
In addition to having their own family plan and educating the families of their patients, pediatricians should address several issues for their offices and staff. These issues involve ensuring the safety of staff and patients, protecting equipment and material, and securing patient records.
Consider the need to have a backup generator to maintain refrigeration for vaccines and other medications. When necessary, plan for a backup location for treating your patients and, if possible, a method for informing callers where they can obtain care. Refer to the American Academy of Pediatrics Online Tool for Disaster Preparedness for Pediatric Practices.
4.2. Planning by Schools
Public and private schools also need emergency response plans.
School plans should include details on how urgent medical care can be provided when needed on site. Plans should include training for school staff in basic life support, first aid, and rescue techniques.
School disaster plans should also address the identification and management of post-traumatic stress in students and staff members, as well as indications for referral for professional psychological intervention.
Following a disaster, children often need the security of a normal routine and support of teachers and peers. Closing schools for a prolonged period negatively impacts the functioning of children after a disaster. Every effort should be made to open schools as soon as possible after an event. Use of school buildings as emergency shelters may hinder or complicate their reopening. Therefore, coordination between schools and relief agencies such as the Red Cross or the local organization for emergency management will assist in the transition to normal operations.
Child care centers also need a plan to ensure the safety of children, to coordinate with other community response agencies, and to provide a method for reuniting children with family members. Child care centers need to educate and train staff members to implement the emergency plan efficiently.
Families, schools, and child care centers must consider how to help children with special health-care needs in an emergency situation. The AAP and the American College of Emergency Physicians have published an emergency information form (EIF) for children with special needs. This document provides important medical information about the child to any person responsible for their emergency medical care.
4.3. Medical Planning for Shelters
Shelters should have an identifiable person who is available, accountable, and responsible for communicating with agencies or organizations for supplies and assistance. Emergency planning must consider the possibility of prolonged shelter use which would require additional supplies and greater attention to organizational details. Planning should include sources of supply and methods of transportation. The needs of pregnant women, infants, and young children must be considered with respect to formula, diapers, basic first aid, hygiene, and safety. Shelters also must consider children with special health-care needs. For example, children with asthma may need nebulizer treatments. Although their families are likely to have brought their own nebulizers, a source of electricity is needed for these devices to operate.
Similarly, a refrigerator is required to store insulin for children and adults who have diabetes. Families with very young or debilitated children may move temporarily to a shelter to protect them from the heat, cold, sun, wind, or rain. Whenever possible, shelter staff members should have direct telephone or radio access to emergency medical care services to obtain medical advice. Ideally, a shelter should have isolation protocols for highly contagious infections such as measles and chickenpox.
Shelter life must also be organized so that children are supervised and have the opportunity for constructive play and entertainment. Supervised activities enable the staff to inform children and keep them safe, while allowing them to participate in activities and tasks. Drawing and other creative activities can help children express themselves and reduce stress. Activities engaging adolescents reduce the potential of adolescent violence and mischief.
Safety in shelters is as important as safety at home. Keep drugs, medical supplies, and potentially dangerous personal items out of children’s reach. Reduce the risk for slips or falls in bathrooms and on all floors.
Lock unoccupied rooms and monitor exits. People residing in shelters should know where the emergency exits are and how they are used. If the shelters allow the possession of weapons, these must be kept out of children’s reach.
4.4. Planning by Hospitals
The WHO comprehensive safe hospital framework provides a guide for preparing hospitals for their role in disaster risk management.
Some guiding principles when applying the framework from the report are as follows:
- Strengthen coordination mechanisms to build and move forward with a national Safe Hospital programme.
A national Safe Hospital programme needs inputs from various sectors, including those beyond the health sector. A comprehensive approach would be best guided by a coordination mechanism that brings together all relevant sectors to address all aspects of the Safe Hospitals programme.
- Build evidence and apply good practices and risk-informed approaches to safe hospitals.
The Safe Hospitals programme should be implemented on the basis of lessons learned from past experience and good practices founded on strong evidence of what works. Lessons, evidence and good practices will be gathered through documentation and research which is an integral part of the programme. Specific approaches will also be shaped by the risks and resources available in the location of implementation.
- Position safe hospitals as a key component of policies and programmes for disaster risk management at national and local levels.
The role of a hospital goes beyond that of a traditional provider of health-care services. The framework builds on the role of hospitals within the disaster risk management system and positions them as key players with the ability either to lead or to strongly support actions taken to build the overall resilience of a country or locality to emergencies and disasters.
- Engage key stakeholders, including communities, in Safe Hospital programmes and activities.
Building a safe hospital requires inputs from different sectors and participants — including architects, structural engineers, water and sanitation experts, health professionals and others. Partnerships between different sectors are vital to ensure that hospitals are constructed safely and can function effectively when an emergency occurs — for instance, by ensuring water and power supplies or securing access to hospitals. It is suggested that a dedicated group of stakeholders from relevant sectors (i.e. health officials, public- and private-sector hospital managers, engineers, architects and national disaster risk management entities) build, implement and manage the programme together to ensure an integrated and comprehensive approach.
- Ensure continuous monitoring and evaluation of the Safe Hospital programme based on a set of agreed indicators.
A mechanism for regular monitoring and evaluation of the impact of the programme should be built into the overall approach
If you work regularly at a hospital, review the hospital disaster plan to ensure that the plan adequately considers the needs of children. If your hospital lacks an emergency plan, offer to help develop a plan. Available resources are listed in Box 4.
BOX 4. Resources for Hospital Disaster Planning
- Occupational Safety and Health Administration at http://www.osha.gov/dts/osta/bestpractices/firstreceivers_hospital.html
- American Academy of Pediatrics – Children & Disasters at https://www.aap.org/en/patient-care/disasters-and-children
Hospital planning for disasters should deal with hospital and pre-hospital events. Hospital events include accidental or non accidental events such as the collapse of hospital structures, fires, explosions, pandemics or toxic exposures. Plans should include a detailed description of the measures taken to protect staff members, patients, and visitors. In cases of infectious diseases or toxic exposures, protective personal equipment and isolation procedures must be instituted immediately to protect staff or other patients. Hospitals may need to coordinate with government agencies to access stockpiles of necessary medicines, vaccines, or equipment. In cases of structural collapse, fire or explosions, rescue interventions attempted by hospital staff who have received no previous training can put them in serious danger. Educate staff about basic safety precautions, and knowing when to intervene or to wait for the arrival of trained rescue workers. During the past 25 years, natural disasters have destroyed dozens of hospitals and hundreds of health centers, resulting in the deaths of thousands of patients, physicians, nurses, and other people who were trapped in the debris.
Hospitals must determine if it is necessary to build their surge capacity. The ability to treat and manage a sudden influx of patients will be determined by a variety of factors including, but not limited to, the number of inpatient, ICU, or emergency beds available, surgical capacity, staffing needs for all departments, supplies, and other physical spaces available for expansion of treatment areas. It is important to ensure that existing inpatients also receive appropriate care and are discharged or transferred to other facilities if necessary. The plan should include a communication method to call in additional health-care professionals and ancillary staff. Directors of hospitals and emergency departments should have a basic knowledge of the local disaster plans and the local command levels. Select one or more members of the hospital staff to serve as liaisons with other responding organizations and agencies to coordinate any activities undertaken outside the hospital environment. In certain situations, a hospital can also serve as shelter for staff members and their families, patients with special needs, and the general public.
CASE 1:
A shelter with 130 evacuates is severely damaged by a tornado during a storm. According to the local protocol, emergency medical services cannot reach the place due to the intensity of the storm. Victims of the tornado, both adults and children, begin to arrive massively to the nearest hospital emergency department. Referrals to other hospitals are not feasible because of the storm.
- Does your hospital disaster plan take into account victims arriving on their own, or does it only consider those transported by the emergency medical services?
- Are emergency department staff members prepared to perform a primary triage of the victims?
- Does your hospital disaster plan take into account the staffing and resources needed to operate under highly demanding conditions with minimal external help?
Some U.S. hospitals have adopted a modified system for mass casualty incidents or disasters that mirrors the external incident command system. Originally known as the Hospital Emergency Incidents Command System (HEICS), it is now known simply as the Hospital Incident Command System (HICS). The system was originally developed by California firefighters in order to establish a common command structure and nomenclature.
This allows for a greater integration with the external response plans (Figure 2 and Box 5) and provides a working command structure for the hospital. It also recognizes the necessity of many other ancillary services and functions that may not be initially considered a part of direct patient care, but are nonetheless vital to emergency hospital operations.
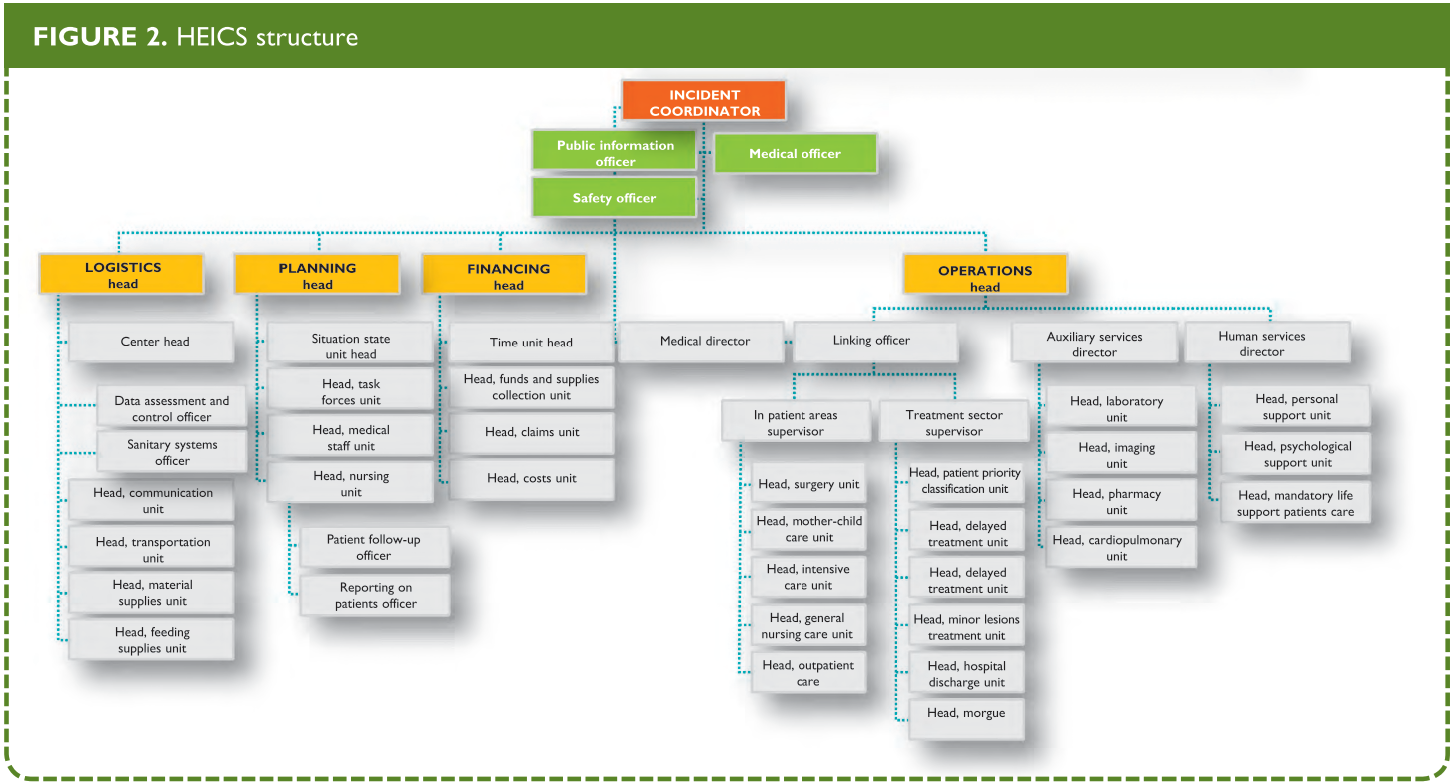
From: Hospital Emergency Incident Command System Update Project. California Emergency Medical Services Authority Web Site.
Hospitals can also offer physicians who have lost their offices a space in which to attend to patients or in turn, provide emergency credentialing to community physicians when additional help is need. These additional physicians can cooperate with the regular hospital physicians in the care of patients who have minor conditions, thereby allowing regular hospital staff to attend to more critical cases.
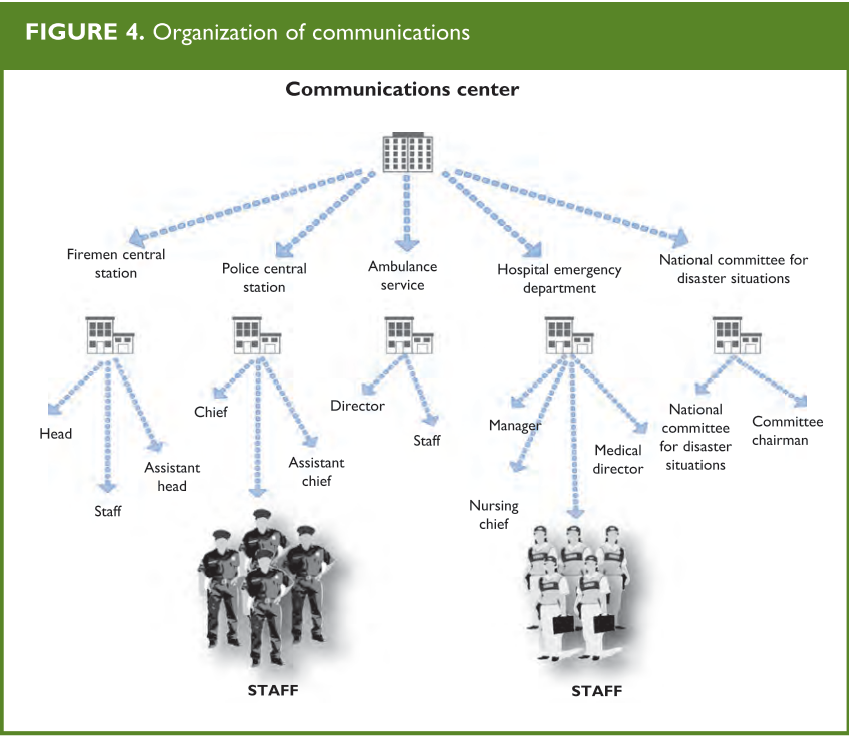
BOX 5. HEICS
HEICS (Hospital Emergency Incident Command System) was created in 1993 in California, by the authorities of San Mateo district medical emergencies service (MES). It consists in an algorithm of positions, the holders of which have a specific task in the event of an emergency situation (Figure 1). Each of these persons has his/her own listing of tasks to be carried out, so that he/she can guide the implementation of these tasks in the framework of an integral system if a disaster occurs. HEICS also includes listings of operations aimed at maximizing the overall efficiency, promoting the undertaking of responsibilities, and facilitating the recording of key data. This system has a flexible structure, allowing the activation of the required positions only, since activating the entire structure may take hours and even days. In the great majority of cases, less than the complete structure will be needed. The listed positions are not assigned to a specific individual; several individuals can be available to cover a position assigned by the incident coordinator; in other cases, a single individual has to undertake more than one position, according to the listing of tasks.
Hospital plans also need to address the management of stress. Frequent rotation of providers and staff during surge times enables efficient performance, and minimizes psychological and physical exhaustion. Hospital plans should also take into consideration the care of individuals with acute stress reactions, those who feel guilty for having survived or having abandoned their families, and those who have suffered considerable material losses or have other psychological sequelae during and after the disaster. Post-traumatic stress disorder and other stress-related syndromes are frequent after a disaster.
4.5. The Emergency Medical Services and Government Planning
Emergency Medical Services (EMS) are a type of emergency service dedicated to providing out-of-hospital acute medical care and/or transport to definitive care to patients with acute illness and injuries. The US has a sophisticated system of EMS agencies that include different levels of providers. Each type of provider is an integral part of the system and the composition of providers is dependent on the needs and resources of the local area.

For pediatric care, EMS must ensure that providers have proper training to take care of children on a daily basis, and are familiar with pediatric dosing, pediatric equipment use, and the needs of children during a disaster. EMS personal should participate in mass-casualty incident drills and exercises involving pediatric patients. Understanding the regional pediatric capabilities, such as the location of pediatric trauma and pediatric burn centers, is necessary. Having appropriate pediatric destination protocols, equipment, and memory aids to respond to the needs of children are important parts of the EMS response.

EMS “DISASTER” Response
- D Detect
- I Incident Command
- S Scene Security and Safety
- A Assess Hazards
- S Support (determine need, order resources early)
- T Triage and Treatment
- E Evacuation and Transport
- R Recovery

Partnerships with federal, state, and local EMS agencies exist to ensure the common goal of protection and preparedness for the states and its citizens. The local community and state leaders are responsible for their own disaster management. The responsibility of the federal government is to provide support, a framework for organization, and resources.
References Websites
5. Mass Casualty Management and Medical Care
Objectives
- Learn the basic components of a mass casualty management approach
- Differentiate the various roles of the individuals providing assistance during a disaster.
- Be familiar with the rescue chain from the incident site to the hospital.
- Understand the importance of patient documentation and recording.
- Understand and apply the triage algorithms.
- Identify the differences between the adult and pediatric triage algorithms (START and JumpSTART).
- Identify the tasks of a mass casualty management approach in humanitarian emergencies.
- Be familiar with the planning tasks during the mitigation phase.
Medical Care in a Mass Casualty Incident (MCI)
Mass casualty management, as may occur in a disaster situation, requires an adjustment of the traditional emergency care approach. In the traditional care approach, first responders are trained to provide victims with basic triage and health-care before evacuation to the nearest available receiving health-care facility. This approach juxtaposes two organizations that work independently with only weak linkages: the field (often involving non health sector responders), and the receiving health-care organization that is often totally divorced from the pre-hospital problem. In a mass casualty situation, this approach will quickly result in chaos. For this reason, a system that would allow an adequate response to mass casualty situations was developed.
CASE 2.
A school bus with primary school students and caregivers leaves for a drive into the countryside, but skids on a sinuous stretch of the road and overturns. The vehicle is seriously damaged. Several children and adults manage to escape, and many remain trapped inside. Children are screaming and crying.
- Are emergency medical care agencies in your district prepared for the rescue, triage, management, and transport of a large number of severely injured children?
- Which of the local hospitals is prepared to provide care to severely injured children?
- Is the nearest trauma center prepared to treat so many patients?
- Will some of the local pediatric emergency departments be able to collaborate in the management of some of the less seriously injured victims?
This system, known as mass casualty management, includes pre-established procedures for resource mobilization, field management, and hospital reception. It is based on specific training of various levels of responders and incorporates links between field and health-care facilities through a command post. It acknowledges the need for a multi-sector response for triage, field stabilization, and evacuation to adapted health-care facilities. The development of this approach is based on the availability of large amounts of human and material resources, so it should be adapted to the available resources to maintain the same effectiveness in its implementation.
The mass casualty management system is based on:
- Pre-established procedures to be used in daily emergency activities and adapted to meet demands of a major incident
- Maximizing usage of existing resources
- Multi-sector preparation and response
- Strong pre-planned and tested coordination
This system is developed to:
- Accelerate and amplify daily procedures to maximize the use of the existing resources
- Establish a coordinated multi-sector rescue chain
- Promptly and efficiently bring disrupted emergency and health-care services back to routine operations.
The rescue chain, the essence of the mass casualty management system, involves the health department, private hospitals, police, fire department, nongovernmental organizations (NgOs), transport services, and communications (Figure 3). This chain starts at the disaster site (with activities such as initial assessment, command and control, search and rescue, field care), continues with transfer of victims to appropriate facilities (using procedures to regulate evacuation and ambulance traffic control), passes through hospital reception (with activation of the hospital disaster response plan), and ends only when the victims have received all emergency care needed to stabilize them.
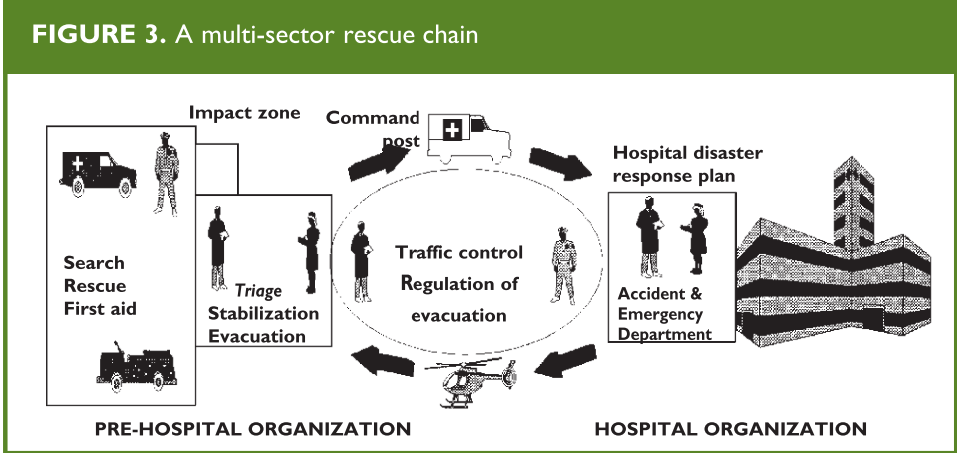
From: Establishing a Mass Casualty Management System, Washington D.C., 1996.
The implementation of this rescue chain requires the following components:
- An efficient emergency department
- A basic radio communications network
- Coordination procedures among all sectors involved
- Skilled multi-sector rescue teams
The assignment and organization of resources in mass casualty management requires careful planning.
As in any chain, the strength and reliability of the system depends on each link; if one fails, the entire system will be compromised.
5.1. Activities at the site of the disaster
These activities include the procedures needed to organize the disaster zone. The alert
given by any observer sets the process into motion. Define exactly the location of the disaster event, the time of its occurrence, its type, the estimated number of victims, the risks, and the population threatened by these risks.
The initial assessment will establish what resources will be mobilized at the site of the disaster (Figure 3).
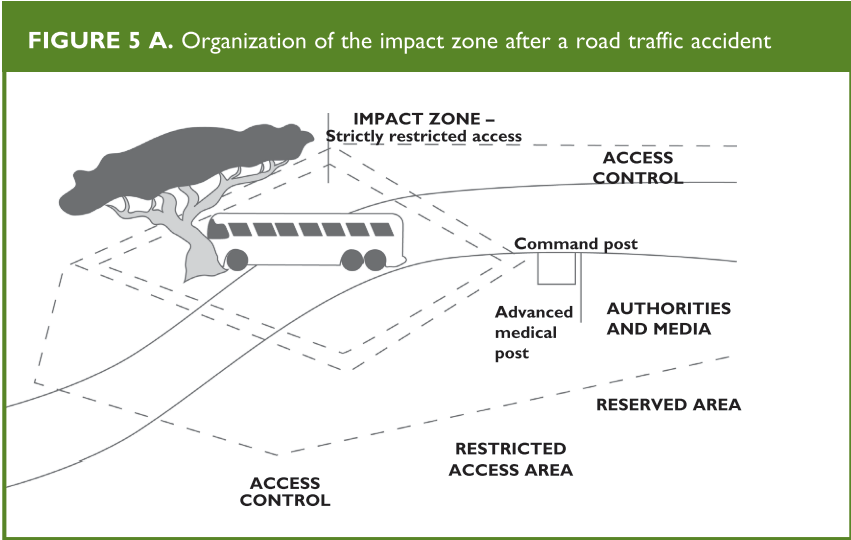
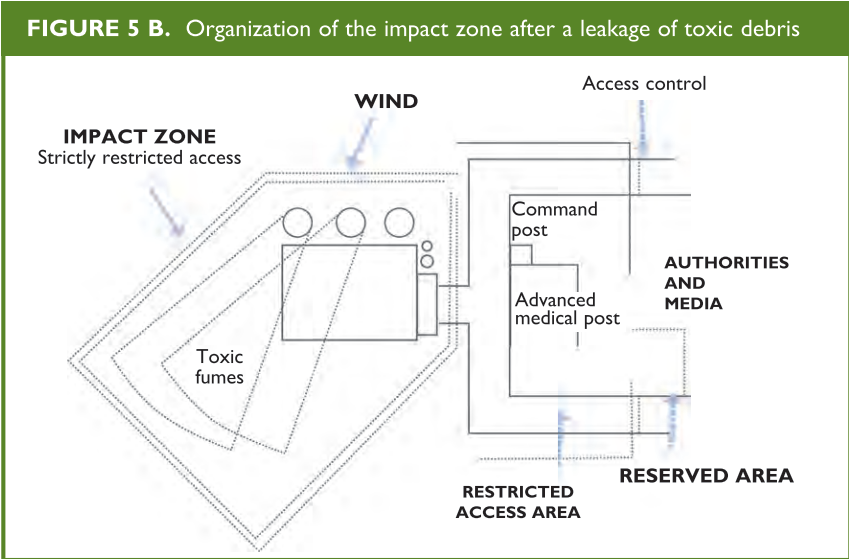
The initial evaluation unit identifies the zones to be set up at the incident site:
- Impact zone
- Incident command post
- Advanced medical post
- Evacuation area
- Authorities and press
- Roads of access
- Restricted areas
(Figures 4 and 5 A and B)
Appendix B, page 39, displays a number of function cards that define in detail the basic
activities of the professionals involved in the coordination and the care of victims in a MCI.
From: Establishing a Mass Casualty Management System, Washington D.C., 1996
Safety
Rescue activities during a disaster should include measures to guarantee the safety of the victims, the members of the rescue units, and the general population.
Communication and documentation
When a disaster occurs, both landline telephones and cell phones could be overburdened.
The communication method of choice for emergency organizations utilize ultra-high frequency (UHF) and very high frequency (VHF) waves. The former are used for communications within the area of the event, and the latter provided from the site to the Incident Command and from there to intervening agencies and the nearest hospital.
for communications with strategic centers for purposes of coordination or transportation. Patient referral information should be provided from the site to the Incident Command and from there to intervening agencies and the nearest hospital. Essential information to be collected includes:
- Number of victims
- Number of persons who need to be transferred to a hospital
- When and how they will be transported
- Relevant lesions care of victims
From: Establishing a Mass Casualty Management System, Washington D.C., 1996.
Care of Victims
Search and rescue activities should be performed by individuals with specific capabilities including firefighters and specialized rescue units. Before allowing these individuals to enter the disaster area, verify whether they need special clothing or breathing equipment to protect them from environmental risks.
Once the search and rescue units have located the victims, they must take them to a risk-free casualty collecting point to be assessed (field triage).
After this initial triage, the victims receive first aid according to their status. When the number of victims or the distance from the place of the incident prevents the direct transportation of all victims to hospitals, an advanced medical post may be established adjacent to, but outside of, the impact zone.
From: Establishing a Mass Casualty Management System, Washington D.C., 1996
Prior to the advanced medical post, all victims are medically triaged (see “Triage: Rationale” below), to identify those who require immediate care.
Following triage classification, victims are referred to the adjacent treatment areas within the advanced medical post where they are stabilized. Stabilization procedures may include advanced airway management fluid therapy to maintain circulation and treat shock, control of hemorrhage, and analgesics. Document the therapies given in the patient’s evacuation report that accompanies the patient to the hospital. In summary, goals of the advanced medical post are to stabilize patients, reassess their condition (retriage), and organize their transportation to the appropriate hospitals. All these tasks have been summarized as the 3 Ts principle: typifying (classifying), treating, and transporting.
Ideally, the advanced medical post should be staffed with trained emergency medicine physicians and nurses; additional physicians such as surgeons and anesthesiologists can be added if available and needed.
Triage - Rationale
Triage is a system that allows establishing priorities for care and transporting in order to save as many lives as possible. It is performed during the rescue phase, and uses priority criteria for the care of patients, distinguishing those requiring immediate stabilization and transport from those who can wait. In a more detailed analysis, triage also allows for identifying patients who need emergency surgery. The primary triage in a MCI consists of a quick evaluation so that all the victims can be examined in a short period of time and decisions can be made regarding treatment priorities.
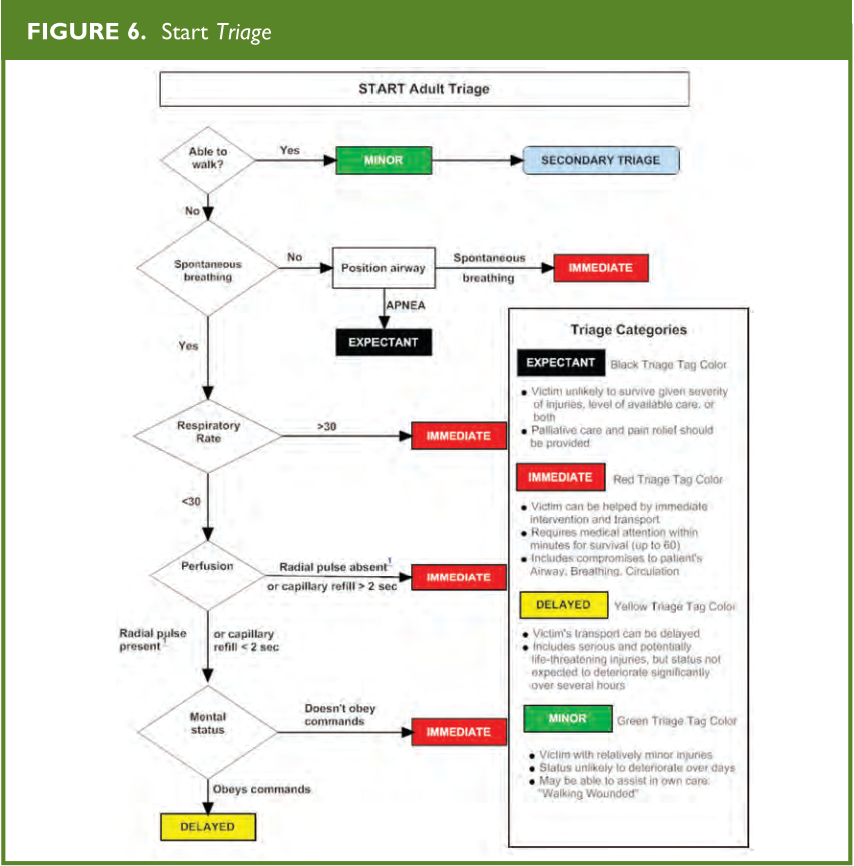
Once the victims are brought to the collection point, the staff responsible for triage must quickly assess each and every victim, and refrain from providing treatment other than hemorrhage control and brief airway repositioning. Specific algorithms, such as the START (Simple Triage and Rapid Treatment, Figure 6) have been used to streamline this process using a color-coding system. START triage evaluates for respirations, pulse/perfusion, and mental status. All patients are triaged first prior to initial medical interventions. During this evaluation, each victim is identified with a specific color-coded tag, tape or marker to indicate the level of medical urgency needed. Primary triage is based on the premise that all the victims are equally important, regardless of age, gender, profession, or any other factor. Decisions are made exclusively based on the victim’s clinical condition. Patients are classified according to severity as green (uninjured or minimally injured), yellow (moderately injured or urgent), Red (severely injured or emergent), and Black (deceased). Field triage is performed on three levels:
On-Site Triage:
Classifies the victims to identify those who need to be taken immediately to the advanced medical post. First aid providers or medical emergency technicians usually do this on-site triage. When the technicians do not have extensive experience in triage, consider having them classify the victims in the “yellow” and “red” groups together as one. Using this approach, the percentage of incorrect classifications declines significantly. In addition, this simplified classification results in a reduction of the time required for the initial evaluation.
Medical Triage:
Determines the required level of care. An emergency physician, anesthesiologist, or surgeon should be in charge of this type of triage.
Medical Triage Classification:
Red: Immediate stabilization is required.
This applies to victims who have:
- Shock due to any cause
- Breathing difficulty with possible respiratory failure
- Profuse external bleeding
- Head trauma with signs of altered consciousness, such as
- disorientation (cannot obey simple commands)
- unconsciousness (cannot respond to verbal and/or painful stimuli)
- asymmetrical pupils (sign of cerebral hernia)
Stabilize these patients so they can receive further care. After stabilization, reclassify.
From: Radiology Emergency Medical Management, https://www.remm.nlm.gov/StartAdultTriageAlgorithm.pdf; adapted from original: Lou Romig, MD
Yellow: Delayed treatment may be appropriate. Monitor closely, insert a line if uncertain about circulatory status, but defer care initially. This category includes victims who, despite not fulfilling the criteria for inclusion in the red group, have:
- Shock risk (e.g., heart attack, abdominal trauma)
- Open fractures
- Femur or pelvis fracture
- Severe burns
- Head trauma but responsive to verbal or painful stimuli
- Uncertain diagnoses
Green: These victims can wait or do not require treatment. This category includes those who are ambulatory and have:
- Minor fractures
- Minor wounds or burns
After on-site care has been completed, transport victims who have been classified as yellow or red to a hospital. They should be re-triaged on arrival.
Black: Deceased.
Evacuation Triage:
Victims are reclassified in terms of their priority for transportation to the nearest hospital.
Red : These victims have the highest priority for transport, preferably with a specialized crew to a tertiary hospital because they require surgery for survival or organ-function preservation or need ICU services.
Yellow : These victims have the second highest priority for transport, which includes victims who are currently stable but may decompensate or require urgent but not emergent surgery.
Green : These victims may be discharged on-site, if possible, after being checked and reassured. Those with minor injuries should be treated or sent to a primary care facility if available.
Black : Transportation to the morgue.
Pediatric triage
The JumpStart triage system is a modified triage algorithm of START based on physiological criteria adapted to the normal range of pediatric values (Figure 7).
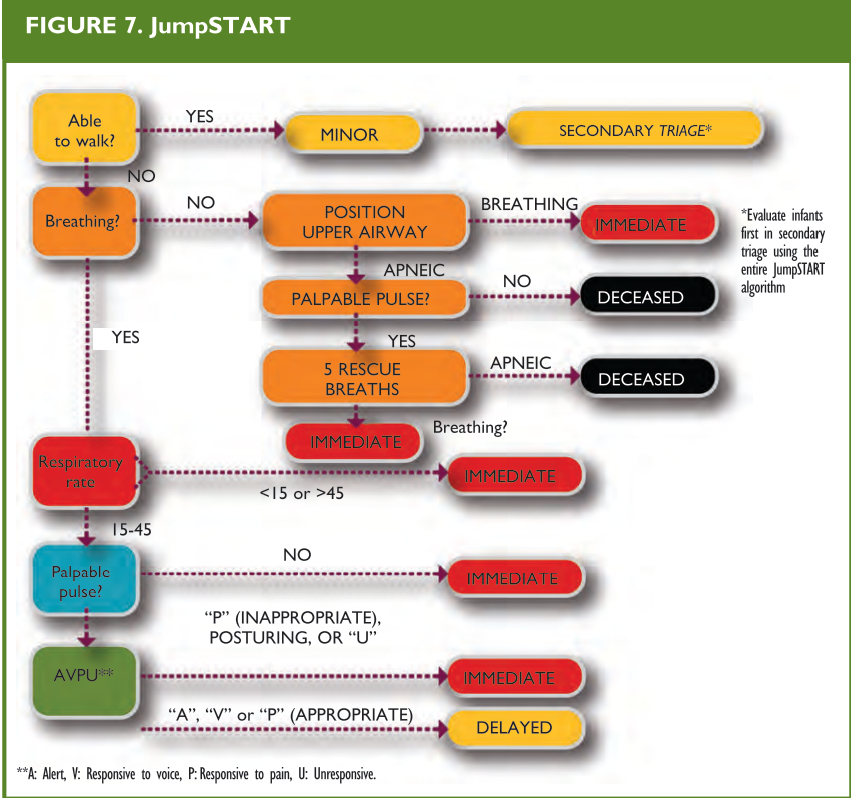
From: Romig LE. Disaster Management. In: APLS Course Manual. Jones & Bartlett Publishers, 2006.
Unlike the adult-based triage system, this system recognizes that an apneic child can still maintain a certain degree of perfusion before he/she develops an irreversible cardiac lesion secondary to anoxia. These children can survive if their respiratory function is sustained or restored, something that will not be identified by applying the START system (Figure 6), which does not include pulse palpation for patients whose apnea persists after the airway has been opened. Children who are not able to walk or are carried in arms by adults should always be categorized at the very least, as yellow.
Regardless of the triage system used, perform a careful secondary evaluation on all the victims on-site and then again at the emergency department. Triage is a dynamic process and continues until the patient arrives at a place where he/she is offered definitive evaluation and treatment.
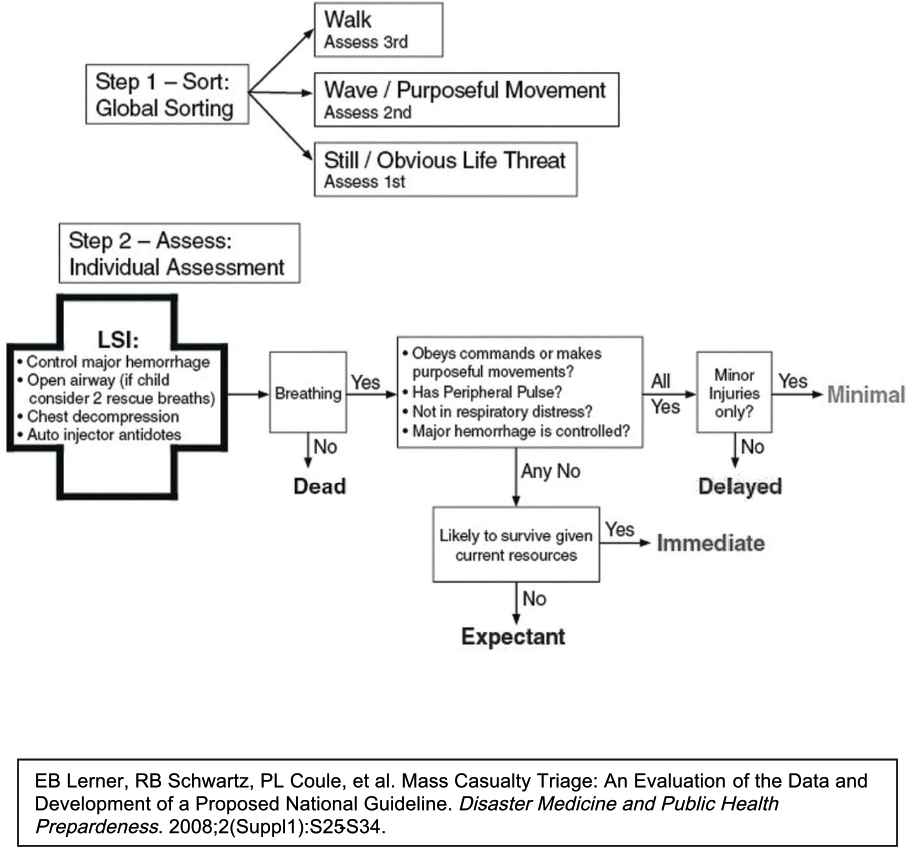
There is a newly proposed national for mass casualty triage called SALT for both adults and children (see Appendix B). SALT stands for “Sort, Assess, Life-saving interventions, and Treatment.” This guideline was developed due to the multiple triage systems, many of which have been inadequately guideline validated. This guideline was developed by an interdisciplinary committee of the AMA, the American College of Surgeons, the American College of Emergency Physicians, the National Association of EMTs, and various other representative organizations.
Global sorting is the first step to address the “walking wounded”. Those who are able to walk are prioritized last; those who cannot follow a command or have an obvious life threat are prioritized first; and those who can follow a command but are unable to walk are prioritized second. The next step of this triage system is to make lifesaving interventions before assigning a patient to a triage category. Lifesaving interventions include control of major hemorrhage, opening the airway and providing 2 breaths for child
casualties, decompression of a tension pneumothorax, and use of autoinjector antidotes. Finally, triage categories are assigned to be Delayed, Immediate, or Expectant management based on breathing, peripheral pulses, respiratory distress, and hemorrhage control. This system of triage is different from the other systems in that there is a grey or “Expectant” category. This category means that the patient may have a life threatening injury, but current resources are not available to meet the demand. The “expectant” category of patients should be re-evaluated frequently as resources become available.
This system of triage does not assign “colors” to patients; therefore, it should not be confused with other triage systems. The SALT triage system is an attempt to take the best features of triage systems that have been tested. It is a different method of triage in that there is global sorting based on the ability to follow commands and walk, and a triage
category assignment based on response to life-saving interventions. Children would likely be over-triaged to the “assess 1st category,” as many will not be capable to follow commands due to developmental stage. This over-triage is probably inherent in pediatrics and can not be avoided. This SALT system of triage should be tested against the most commonly used form of pediatric triage: Jump START.
5.2. Transfer organization
The transfer organization includes those procedures implemented to ensure that victims of a mass casualty incident will be safely, quickly, and efficiently transferred by appropriate vehicles to a prepared healthcare facility.
Transfer is organized according to different principles such as strict control of the rate and destination of evacuation to avoid overwhelming the health-care facilities. One of the roles of on-scene mass casualty management is to stop spontaneous evacuation from by-standers of unstable victims or those minimally injured. This unmanaged transport is unsafe, endangers the lives of victims, circumvents field decontamination process, and disrupts the implementation of the mass casualty management system. Victims should not be removed from the advanced medical post to health-care facilities before:
- They are in the most stable condition possible.
- They are adequately equipped for the transfer.
- The receiving health-care facility is correctly informed and ready to receive the patient.
- The most appropriate vehicle and escort are available
Control of Victim Flow: The Noria Principle
Patient movement (whether by walking, by stretcher, or by vehicle) must be in a “oneway” direction and without any back-tracking. From the impact zone to the collecting point, from the collecting point to the advanced medical post entrance, and subsequently to areas of treatment, evacuation, and hospital care, the victims will be on a one-way “conveyor belt”, taken from the scene to sophisticated levels of care (Figure 8)
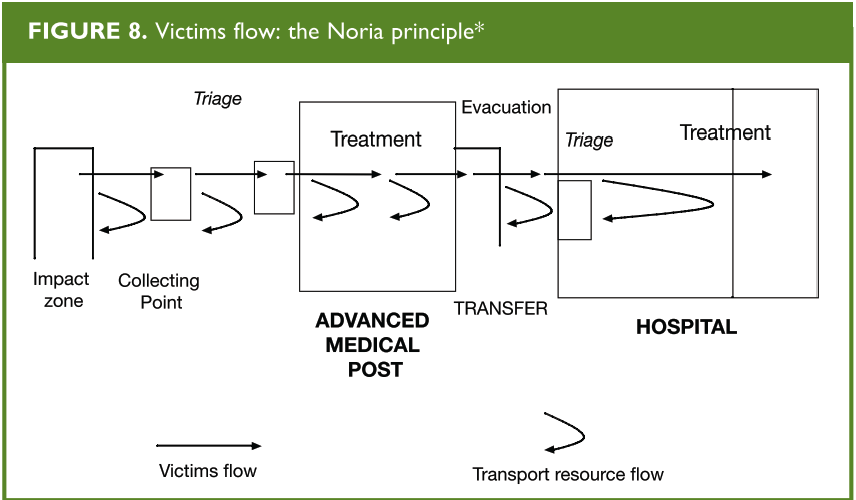
*This one-way progression from level to level by rotating transportation resources was labelled “Noria” in 1916 during the World War I battle of Chemin de Dames in Verdun, France. “Noria” comes from the Latin word for “wheel”. From: Establishing a Mass Casualty Management System, Washington D.C., 1996.
5.3. Organization of Hospitals
The mass casualty management system needs specific organization at the receiving hospital. This organization allows the active mobilization and management of available or needed resources, communicates with pre-hospital providers, and facilitates the management of inpatients and the flow of incoming victims. Other management tasks include secondary evacuations, departments, operating rooms, laboratory, radiology, and intensive care unit, have to be reinforced. It is also important to prepare sequential reinforcements and allow a rapid rotation of the staff in those areas where the workload will be most demanding. This prevents overburdening the staff during an influx of casualties and ensures the prompt return to normal operations with an adequate staff.
As part of the coordinated efforts, hospital security should be reinforced with police officers stationed at the gates and in the reception area. In every hospital, there should be a well-equipped command post for use in emergency situations.
Reception of victims
In order to accommodate the influx of new patients, discharge all patients that can be cared for on an outpatient basis. Adding hallway beds or opening up inhospital clinics can help with surge capacity. If victims bypass the on-scene medical triage and arrive at the hospital on their own, they should be triaged appropriately as with any other arriving victim. When prehospital management has been efficient, an experienced emergency nurse can do the triage. If this is not the case, triage should be performed by an experienced emergency physician, anesthesiologist or surgeon. All arriving victims, whether or not they’ve been previously triaged, should be re-triaged upon arrival to the hospital.
Treatment Areas
Clearly establish the treatment areas in the hospital and provide the necessary staffing. Treatment area designation should reflect triage levels, e.g., red treatment area for victims triaged in the red category. An emergency medicine physician or an anesthesiologist should be in charge of the red treatment area and should be prepared to treat patients with extremely severe injuries. An additional triage can determine the order of these red patients that need operative interventions. Victims triaged as yellow should be reevaluated by a physician and provided care or observation as needed. If their condition worsens, transfer them to the red treatment area. Victims with no hope for survival require only supportive care. These patients should be kept in a separate ward. Have an area ready for deceased victims if the hospital morgue is overwhelmed.
6. Summary
Planning is essential to reduce risks and minimize dangers in the event of a disaster. It should be carried out at different levels, from the family unit to the local community with its various entities. Each community should develop its own local emergency or disaster plan. This local disaster plan needs to be adequately coordinated with the regional and national-level plans. Disaster plans should contemplate the basic needs of the affected individuals and the potential displacement of many people which may result in public health risks. The basic components of a disaster plan are: analysis of the situation, assumptions, goals, objectives, site organization, roles and responsibilities, coordination, and recording of critical information. The plan needs a realistic appraisal of available resources and extensive training and coordination.
In responding to a mass casualty incident, a management system should be instituted which includes the command post, the advanced medical post, evacuation and transport, and hospital care. This system must be activated in a coordinated manner, and each component sector should be prepared to organize patient care. All lessons learned during the immediate response to the disaster should be incorporated in future planning.
7. Suggested Reading
- Benson M, Koenig KL, Schultz CH. Disaster triage: START then SAVE-a new method of dynamic triage for victims of a catastrophic earthquake. Prehospital Disaster Med 1996; 11 (2): 117-124.
- Committee on Pediatric Emergency Medicine. The pediatrician’s role in disaster preparedness. Pediatría I997;99(I):I3O-I33.
- Farmer JC, Jiménez EJ, Rubinson L, Talmor DS (eds). Fundamentals of Disaster Management. Society of Critical Care Medicine, 2003.
- Hospital Emergency Incident Command System Update Project. California Emergency Medical Services Authority Web Site.
- Jacob J. Disaster plan can safeguard your practice, records. American Medical Association Web site.
- Lerner et al. Mass Casualty Triage: An evaluation of the data and development of a proposed national guideline. Disaster Medicine and Public Health Preparedness 2(1):S25-S34.
- Markenson, D, Reynolds, S. The Pediatrician and Disaster Preparedness. Pediatrics 117(2) : e340-e362.
- Mothershead JL et al. Disaster Planning.
- Establishing a Mass Casualty Management System, Pan American Health Organization, 1996.
- Humanitarian Assistance in Disaster Situations: A Guide for Disaster Aid. Pan American Health Organization, 1999.
- Safe Hospitals: A Collective Responsibility. A Global Measure of Disaster Reduction, Pan American Health Organization/World Health Organization.
- Romig LE. Disaster Management. In: APLS Course Manual. Jones & Bartlett Publishers, 2006.
- Romig LE. Pediatric triage: a system to JumpSTART your triage of young patients at MCIs. JEMS 2002;27(7):52-63.
- Savage, PE. Disasters. Hospital Planning. Oxford, Pergamon Press, 1979.
8. Case resolution
Case 1.
The hospital disaster plan is activated while all victims are sent to a triage area set up in a safe location (e.g., hospital parking lot). A physician, accompanied by nurses from the emergency department, initiates triage. Patients with critical illnesses or trauma are transported directly to the emergency department. Those most severely affected are treated in the emergency department and receive immediate evaluation, while those with less severe injuries are given first aid in the parking lot or wait until they can be treated in the emergency department. The hospital disaster plan includes utilizing staff from other hospital departments to assist in the event of a mass casualty incident.
Case 2:
The local emergency system verifies the incident, declares a mass casualty situation, and then activates the emergency plan, setting into motion the necessary agencies such as fire, police, and emergency medical services. A structure for the care of victims is established, and children and adults are triaged. An on-scene command post is established. Local hospitals are contacted to inquire about their respective patient care capabilities. All the children with moderate to severe lesions are referred to the nearest pediatric trauma center, whereas adults with moderate to severe lesions are sent to an adult trauma center. After all the severely injured victims have been transported, those patients with minor lesions are referred to primary care facilities.
9. Module Review
SECTION I: LOCAL EMERGENCY PLAN
- What are the pediatrician’s specific functions in a disaster plan?
- What factors should be considered when designing a local plan?
- What areas should the plan cover?
- What is the desired profile for the emergency plan coordinator, and what roles should he/she play?
SECTION II: PLANNING LEVELS
- Planning should cover several levels. What are these levels, and what are the components and the adequate methods in each case?
- What individual and family factors should be taken into account in a disaster situation?
- What role do community organizations play in the sequential phases of a disaster situation?
- How should these organizations be equipped to face the problems that affect children which may be directly or indirectly related to the disaster?
SECTION III: MASS CASUALTY MANAGEMENT AND MEDICAL CARE
- What are the basic components of a mass casualty management system?
- How is a command post for a MCI established? What areas should be defined around the site of impact?
- How is an advanced medical post organized?
- What are the roles of the individuals involved in the emergency medical care chain? How are these roles determined?
- At which points in the rescue chain is triage performed, and what priorities are established in each case?
- What special conditions should be considered when triaging a pediatric victim? How are these conditions integrated in a MCI where victims are not only children?
- What data are essential for the internal communication within the system? How are these data transmitted?
- What elements should be considered when organizing the transportation of victims to hospitals and other healthcare centers?
- What systems of hospital care can be used in the response to MCI? How do these systems operate?
- What planning aspects correspond to the mitigation phase?
10. Appendix A: Roles and Responsibilities of ESFs
ESF #1 – Transportation
- Aviation/airspace management and control
- Transportation safety
- Restoration/recovery of transportation infrastructure
- Movement restrictions
- Damage and impact assessment
ESF #2 – Communications
- Coordination with telecommunications and information technology industries
- Restoration and repair of telecommunications infrastructure
- Protection, restoration, and sustainment of national cyber and information technology resources
- Oversight of communications within the Federal incident management and response structures
ESF #3 – Public Works and Engineering
- Infrastructure protection and emergency repair
- Infrastructure restoration
- Engineering services and construction management
- Emergency contracting support for life-saving and life-sustaining services
ESF #4 – Firefighting
- Coordination of Federal firefighting activities
- Support to wildland, rural, and urban firefighting operations
ESF #5 – Emergency Management
- Coordination of incident management and response efforts
- Issuance of mission assignments
- Resource and human capital
- Incident action planning
- Financial management
ESF #6 – Mass Care, Emergency Assistance, Housing, and Human Services
- Mass care
- Emergency assistance
- Disaster housing
- Human services
ESF #7 – Logistics Management and Resource Support
Comprehensive, national incident logistics planning, management, and sustainment capability
Resource support (facility space, office equipment and supplies, contracting services, etc.)
ESF #8 – Public Health and Medical Services
- Public health
- Medical
- Mental health services
- Mass fatality management
ESF #9 – Search and Rescue
- Life-saving assistance
- Search and rescue operations
ESF #10 – Oil and Hazardous Materials Response
- Oil and hazardous materials (chemical, biological, radiological, etc.) response
- Environmental short- and long-term cleanup
ESF #11 – Agriculture and Natural Resources
- Nutrition assistance
- Animal and plant disease and pest response
- Food safety and security
- Natural and cultural resources and historic properties protection and restoration
- Safety and well-being of household pets
ESF #12 – Energy
- Energy infrastructure assessment, repair, and restoration
- Energy industry utilities coordination
- Energy forecast
ESF #13 – Public Safety and Security
- Facility and resource security
- Security planning and technical resource assistance
- Public safety and security support
- Support to access, traffic, and crowd control
ESF #14 – Long-Term Community Recovery
- Social and economic community impact assessment
- Long-term community recovery assistance to States, local governments, and the private sector
- Analysis and review of mitigation program implementation
ESF #15 – External Affairs
- Emergency public information and protective action guidance
- Media and community relations
- Congressional and international affairs
- Tribal and insular affairs
11. Appendix B: Function Cards
PAHO has created a number of function cards that define in detail the basic activities of the professionals involved in the coordination and the care of victims in a MCI.
1. Operator - dispatch center
- Receives initial call or warning message concerning the event
- Establishes: caller’s name and telephone number - nature of event - exact location of event - time of occurrence - approximate number of victims
- Verifies information (if an unqualified observer)
- Mobilizes and sends a dispatch team to site for initial assessment
- Alerts potential responders (stand by)
- Receives report of initial assessment
- Dispatches necessary resources
2. Initial assessment team
- Travel to site expeditiously
- Identify a leader
- Establishes: precise location of the event time of the event - type of incident
- Estimates: number of casualties - added potential risk - exposed population
- Team Leader reports initial information to dispatch center
- Draws a single map of the area indicating:
- main topographical features
- potential risk areas
- victims
- access roads various field areas
- limits of restricted areas
- compass rose
- wind direction
- Directs resources arriving in the field until the arrival of a high ranking officer
- Hands over the map and briefs first arriving officer of rank
- Reports to reassigned station
3. Fire services
The Fire Services will be responsible for:
- Safety
- Search and rescue
- Risk reduction
- Definition of restricted areas
- Providing a senior officer as a staff member of the Command Post
- Providing the Advanced Medical Post (AMP) with a Transport Officer
4. Search and rescue team
- Locates victims
- Removes victims from unsafe locations to collection point if necessary
- Conducts initial triage of victims (acute/ nonacute)
- Provides essential first aid
- Transfers victims to Advance Medical Post
5. Search and rescue officer
- Coordinates search and rescue activities by:
- identifying and assigning teams supervising team functioning
- establishing a collection point when necessary coordinating the transfer of patients from the collection point to the Advance Medical Post communicating with Command Post for resource reinforcement
- ensuring safety and welfare of search and rescue teams
6. Coordinator of the command post
- Performs overall coordination of the field operations
- Receives reports from the other officers in the Command Post
- Continuously assesses the general situation
- Coordinates requests between sectors in the field
- Ensures links between sectors
- Ensures the welfare of all staff involved in field operations
- Liaises with central headquarters, (e.g., EOCs)
- Authorizes releases to the media
- Acts as link between field operations and backup system
- Acts as link between field operations and backup system
7. Fire officer in command post
- Coordinates activities of the Fire Service in the field (ensures safety, search and rescue)
- Assists in transport organization
- Manages fire staff resource needs by:
- continuous assessment
- requests for backup
- timely rotation of staff withdrawal of staff no longer needed
- Reports to the coordinator of the Command Post
8. Police officer in command post
- Ensures that radio communication is established and maintained
- Implements security measures to:
- maintain restricted areas
- provide crowd and traffic control
- Manage field police resources by:
- continuous assessment of needs
- redeployment of police officers
- requests for backup
- ensure adequate supply of necessary equipment
- This officer is generally the coordinator of the Command Post
9. Health officer in command post
- Supervises the field care of victims
- Provides the link between the health/ medical backup system
- Ensures the adequate supply of manpower and equipment
- Receives reports from the manager of the Advance Medical Post (acute treatment manager)
- Deploys and manages health staff resources
- Reports to the coordinator of the Command Post
10. Acute treatment manager (manager of advance medical post)
- Supervises triage and stabilization of victims in AMP
- Establishes the internal organization of the AMP
- Manages the staff of the AMP
- Ensures that effective victim flow is maintained
- Ensures adequate equipment and supplies are available in each treatment area
- Organizes the transfer of patients to health care facilities in collaboration with the Transport Officer, the Health Officer in the Command Post and receiving Health Care facility
- Decides on the transfer order of victims, the mode of transport, escort and destination
- Ensures staff welfare
- Reports to the Health Officer in the Command Post
11. Medical triage officer
- Receives victims at the entrance of the AMP
- Examines and assesses the condition of each victim
- Categorizes and tags patients as follows
- Red-immediate stabilization necessary
- Yellow-close monitoring, care can be delayed
- Green-minor delayed treatment or no treatment
- Black-deaths
- Directs victim to appropriate treatment area
- Reports to the manager of the AMP
12. Red team leader
- Receives patient from medical triage
- Examines and assesses the medical condition of the victim
- Institutes measures to stabilize the victim
- Continuously monitors victim’s condition
- Reassesses and transfers victims to other treatment areas
- Prioritizes victims for evacuation
- Requests evacuation in accordance with priority list
- Reports to the manager of the AMP
13. Evacuation officer
- Receives victims for evacuation
- Assesses the victim’s stability
- Assesses the security of any equipment attached to victims and corrects deficiencies
- Ensures that immobilization is adequate
- Ensures that the tag is safely and clearly attached
- Maintains observation of victims until transported
- Supervises loading and ensure escort is briefed
- Reports to manager of AMP
14. Transport officer
- Coordinates and supervises the transportation of victims
- Identifies access routes and communicates traffic flow to drivers
- Supervises all available ambulance drivers and drivers of assigned vehicles
- Receives requests for transportation
- Assigns appropriate vehicle tasks in accordance with specific needs
- Maintains a log of the whereabouts of all vehicles under his control
- Reports to the manager of the AMP
15. Administration clerk - triage area
- Maintains a register of all victims admitted to medical triage
- Records
- name or identification number
- age when possible
- sex
- time of arrival
- injury category assigned
- Reports to Triage Officer
16. Administration clerk evacuation area
- Maintains a register of all victims leaving the AMP
- Records
- victim name/number
- injury category
- time of departure
- mode of departure (vehicle) and escort destination
- Reports to the evacuation office
17. Ambulance driver
- Remains in the vehicle at all times
- Responds promptly to directives from Transport Officer
- Ensures that vehicle is parked in designated area and is ready to move
- Transports patients in accordance with safety rules and instructions
- Reports to Transport Officer
12. Appendix C: Salt Diagram