Pediatric Trauma
5. Disaster Specific Traumatic Injuries
5.1. Special Situations
Electrical Injury
Low-and intermediate-voltage exposures can cause locally destructive injuries, as well as systemic complications. High-voltage exposures cause delayed neurologic and ocular sequelae. It is necessary to serially examine injured extremities for intracompartmental edema requiring decompression. Place bladder catheters to document and treat myoglobinuria.
Chemical Injury
Irrigate the wounds with abundant clean water (isotonic crystalloid for eye globe injuries). Close monitoring of electrolytes is necessary.
Tar Injury
Water irrigation is initially needed to cool molten tar and stop the burning process. Then, remove the cooled tar with lipophylic solvent during the debriding process.
Overall, prompt management of burn patients—with careful monitoring of airway, fluids and electrolytes, and clinical status—will directly impact morbidity and mortality. Definitive management will be determined by the degree of injury, concomitant injuries, and availability of resources.
In a disaster situation with many burned victims and poor resources, priority should be given to admitting children with a burned surface area of more than 10%, those having the face, the hands, the feet and the perineum burned, those having joints burned and circumferential injuries, and those that can't be treated out of hospital for these or other injuries. It is wise to try to establish at least one IV access in patients with burns of more than 10% body surface areas and start fluid replacement with crystalloid 20 ml/kg.
Burns affecting the airway need on site urgent interventions, such as protection of the airway and fluid administration.
Pain should be managed with painkillers and sedatives, titrating doses to the desired effect. The patient should be transferred as soon as possible. When transportation is delayed or prolonged, consult the Burn Department of the reference hospital to establish the rate of intravenous fluid replacement.
Blast Injury
Bombs and explosives can cause distinctive injuries. Survivors of an explosion typically suffer both penetrating and blunt trauma injuries. Blast lung is the most common lethal injury. Half of all initial casualties will seek medical care over a one-hour period.
The upside-down triage triangle (▽) is a reminder that the least sick will arrive at the hospital first, whereas those who are sicker, trapped, closer to the explosion site, or unable to ambulate will arrive later after rescue and in smaller numbers.
Explosives can be classified as either high-order (HE) or low-order (LE). Highorder explosives, such as TNT, C-4, nitroglycerin, or ammonium cause a supersonic over-pressurization shock wave. Loworder explosives, such as black powder or nitrocellulose cause a subsonic explosion.
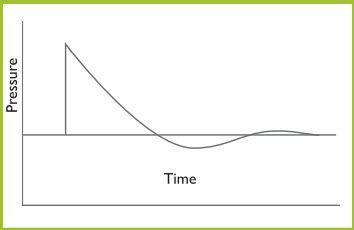
Most of the injuries seen after HE detonations are blunt, penetrating, and thermal trauma. Soft-tissue and head injuries are the most common injuries. Orthopedic injuries are also common. Primary blast injury is a less common, often subtle or delayed potentially life-threatening problem that must be considered. It is a result of abrupt pressure changes generated by the blast wave. As the Friedlander curve shows, a blast wave generates a shock wave that expands spherically. There is an instantaneous rise to a peak over-pressure that declines exponentially to an under-pressure (zone behind the high-pressure blast) (Figure 14). The rapid pressure change is the cause of the primary blast injury. Both high -and low- pressure changes can cause injury.
Figure 14. Friedlander Curve