Planning and Triage in the Disaster Scenario
4. Planning Levels
4.4. Planning by Hospitals
The WHO comprehensive safe hospital framework provides a guide for preparing hospitals for their role in disaster risk management.
Some guiding principles when applying the framework from the report are as follows:
- Strengthen coordination mechanisms to build and move forward with a national Safe Hospital programme.
A national Safe Hospital programme needs inputs from various sectors, including those beyond the health sector. A comprehensive approach would be best guided by a coordination mechanism that brings together all relevant sectors to address all aspects of the Safe Hospitals programme.
- Build evidence and apply good practices and risk-informed approaches to safe hospitals.
The Safe Hospitals programme should be implemented on the basis of lessons learned from past experience and good practices founded on strong evidence of what works. Lessons, evidence and good practices will be gathered through documentation and research which is an integral part of the programme. Specific approaches will also be shaped by the risks and resources available in the location of implementation.
- Position safe hospitals as a key component of policies and programmes for disaster risk management at national and local levels.
The role of a hospital goes beyond that of a traditional provider of health-care services. The framework builds on the role of hospitals within the disaster risk management system and positions them as key players with the ability either to lead or to strongly support actions taken to build the overall resilience of a country or locality to emergencies and disasters.
- Engage key stakeholders, including communities, in Safe Hospital programmes and activities.
Building a safe hospital requires inputs from different sectors and participants — including architects, structural engineers, water and sanitation experts, health professionals and others. Partnerships between different sectors are vital to ensure that hospitals are constructed safely and can function effectively when an emergency occurs — for instance, by ensuring water and power supplies or securing access to hospitals. It is suggested that a dedicated group of stakeholders from relevant sectors (i.e. health officials, public- and private-sector hospital managers, engineers, architects and national disaster risk management entities) build, implement and manage the programme together to ensure an integrated and comprehensive approach.
- Ensure continuous monitoring and evaluation of the Safe Hospital programme based on a set of agreed indicators.
A mechanism for regular monitoring and evaluation of the impact of the programme should be built into the overall approach
If you work regularly at a hospital, review the hospital disaster plan to ensure that the plan adequately considers the needs of children. If your hospital lacks an emergency plan, offer to help develop a plan. Available resources are listed in Box 4.
BOX 4. Resources for Hospital Disaster Planning
- Occupational Safety and Health Administration at http://www.osha.gov/dts/osta/bestpractices/firstreceivers_hospital.html
- American Academy of Pediatrics – Children & Disasters at https://www.aap.org/en/patient-care/disasters-and-children
Hospital planning for disasters should deal with hospital and pre-hospital events. Hospital events include accidental or non accidental events such as the collapse of hospital structures, fires, explosions, pandemics or toxic exposures. Plans should include a detailed description of the measures taken to protect staff members, patients, and visitors. In cases of infectious diseases or toxic exposures, protective personal equipment and isolation procedures must be instituted immediately to protect staff or other patients. Hospitals may need to coordinate with government agencies to access stockpiles of necessary medicines, vaccines, or equipment. In cases of structural collapse, fire or explosions, rescue interventions attempted by hospital staff who have received no previous training can put them in serious danger. Educate staff about basic safety precautions, and knowing when to intervene or to wait for the arrival of trained rescue workers. During the past 25 years, natural disasters have destroyed dozens of hospitals and hundreds of health centers, resulting in the deaths of thousands of patients, physicians, nurses, and other people who were trapped in the debris.
Hospitals must determine if it is necessary to build their surge capacity. The ability to treat and manage a sudden influx of patients will be determined by a variety of factors including, but not limited to, the number of inpatient, ICU, or emergency beds available, surgical capacity, staffing needs for all departments, supplies, and other physical spaces available for expansion of treatment areas. It is important to ensure that existing inpatients also receive appropriate care and are discharged or transferred to other facilities if necessary. The plan should include a communication method to call in additional health-care professionals and ancillary staff. Directors of hospitals and emergency departments should have a basic knowledge of the local disaster plans and the local command levels. Select one or more members of the hospital staff to serve as liaisons with other responding organizations and agencies to coordinate any activities undertaken outside the hospital environment. In certain situations, a hospital can also serve as shelter for staff members and their families, patients with special needs, and the general public.
CASE 1:
A shelter with 130 evacuates is severely damaged by a tornado during a storm. According to the local protocol, emergency medical services cannot reach the place due to the intensity of the storm. Victims of the tornado, both adults and children, begin to arrive massively to the nearest hospital emergency department. Referrals to other hospitals are not feasible because of the storm.
- Does your hospital disaster plan take into account victims arriving on their own, or does it only consider those transported by the emergency medical services?
- Are emergency department staff members prepared to perform a primary triage of the victims?
- Does your hospital disaster plan take into account the staffing and resources needed to operate under highly demanding conditions with minimal external help?
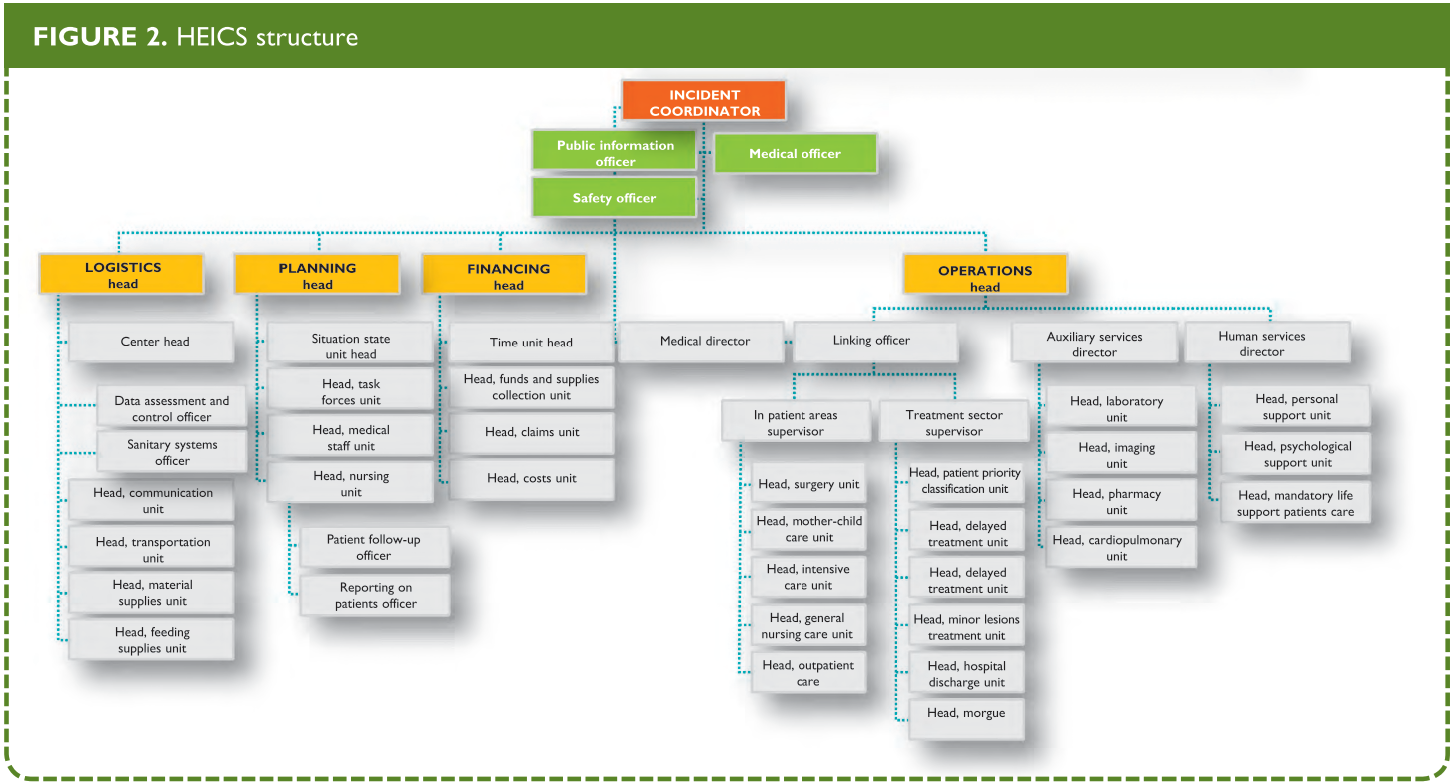
Some U.S. hospitals have adopted a modified system for mass casualty incidents or disasters that mirrors the external incident command system. Originally known as the Hospital Emergency Incidents Command System (HEICS), it is now known simply as the Hospital Incident Command System (HICS). The system was originally developed by California firefighters in order to establish a common command structure and nomenclature.
This allows for a greater integration with the external response plans (Figure 2 and Box 5) and provides a working command structure for the hospital. It also recognizes the necessity of many other ancillary services and functions that may not be initially considered a part of direct patient care, but are nonetheless vital to emergency hospital operations.
From: Hospital Emergency Incident Command System Update Project. California Emergency Medical Services Authority Web Site.
Hospitals can also offer physicians who have lost their offices a space in which to attend to patients or in turn, provide emergency credentialing to community physicians when additional help is need. These additional physicians can cooperate with the regular hospital physicians in the care of patients who have minor conditions, thereby allowing regular hospital staff to attend to more critical cases.
BOX 5. HEICS
HEICS (Hospital Emergency Incident Command System) was created in 1993 in California, by the authorities of San Mateo district medical emergencies service (MES). It consists in an algorithm of positions, the holders of which have a specific task in the event of an emergency situation (Figure 1). Each of these persons has his/her own listing of tasks to be carried out, so that he/she can guide the implementation of these tasks in the framework of an integral system if a disaster occurs. HEICS also includes listings of operations aimed at maximizing the overall efficiency, promoting the undertaking of responsibilities, and facilitating the recording of key data. This system has a flexible structure, allowing the activation of the required positions only, since activating the entire structure may take hours and even days. In the great majority of cases, less than the complete structure will be needed. The listed positions are not assigned to a specific individual; several individuals can be available to cover a position assigned by the incident coordinator; in other cases, a single individual has to undertake more than one position, according to the listing of tasks.
Hospital plans also need to address the management of stress. Frequent rotation of providers and staff during surge times enables efficient performance, and minimizes psychological and physical exhaustion. Hospital plans should also take into consideration the care of individuals with acute stress reactions, those who feel guilty for having survived or having abandoned their families, and those who have suffered considerable material losses or have other psychological sequelae during and after the disaster. Post-traumatic stress disorder and other stress-related syndromes are frequent after a disaster.